CASE 38
FG is a 62-year-old man who had received a renal transplant 12 years earlier after a period of 5 years during which he had undergone both peritoneal dialysis and later hemodialysis. The underlying cause of his chronic renal failure was believed to be a combination of diabetes (he had been insulin dependent since the age of 16) and long-standing hypertension (>25 years), which had been refractory to simple therapy and required triple therapy for adequate control. He has been on maintenance therapy (rapamycin and azathioprine) for immunosuppression, having been weaned from an earlier regimen of cyclosporine and prednisone at the suggestion of his transplant team, who thought this would be a simpler regimen for him.
QUESTIONS FOR GROUP DISCUSSION
RECOMMENDED APPROACH
Implications/Analysis of Family History
Although we are not provided with any family history, this patient has had insulin-dependent diabetes and hypertension for decades. Disease susceptibility for type 1 diabetes mellitus depends on the degree of genetic similarity that an individual has with the proband (see Case 24). Hypertension is known to have a strong genetic association, but the genes have not been identified. There are a number of risk factors for development of hypertension, one of which is diabetes.
Implications/Analysis of Clinical History
Complications of Immunosuppressive Therapy
Complications of the immunosuppressive therapy used to ensure graft survival are unfortunately quite common and include malignancy (lymphoma and melanoma), infection, and drug toxicity. Recrudescence of earlier infections or opportunistic infections can also cause problems in immunosuppressed individuals. Opportunistic infections that could certainly be of concern include Pneumocystis carinii (jiroveci) pneumonia (PCP) and infection with Cryptosporidium, Mycobacterium tuberculosis, as well as the opportunistic species M. avium. Indeed, a variety of pathogens seen in another population of immunosuppressed individuals (e.g., acquired immunodeficiency syndrome; see Case 13) is of more than passing interest as we remember that this patient first came to attention with evidence of liver disease (jaundice).
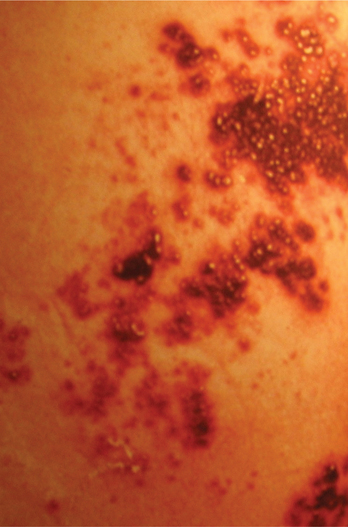
A number of viral infections are also prevalent in immunosuppressed individuals. These include cytomegalovirus (CMV/human herpesvirus 6), hepatitis C, Epstein-Barr virus (EBV/human herpesvirus 4), and human herpes simplex virus (HSV/human herpesvirus 1/2), although the latter two are less likely to cause this hepatitis. Recrudescence of chickenpox (herpes zoster) may also occur in immunosuppressed individuals (Fig. 38-1).