Procedure 37 Duplicated Thumb Reconstruction
 See Video 31: Duplicated Thumb Reconstruction
See Video 31: Duplicated Thumb Reconstruction
Indications
 The goal of thumb reconstruction is to restore an acceptable appearance without compromising existing function. Although a child with thumb duplication can function perfectly without reconstruction, the stigma associated with an uncorrected deformity may be unacceptable for the child or the parents, or both.
The goal of thumb reconstruction is to restore an acceptable appearance without compromising existing function. Although a child with thumb duplication can function perfectly without reconstruction, the stigma associated with an uncorrected deformity may be unacceptable for the child or the parents, or both.

Examination/Imaging
Clinical Examination
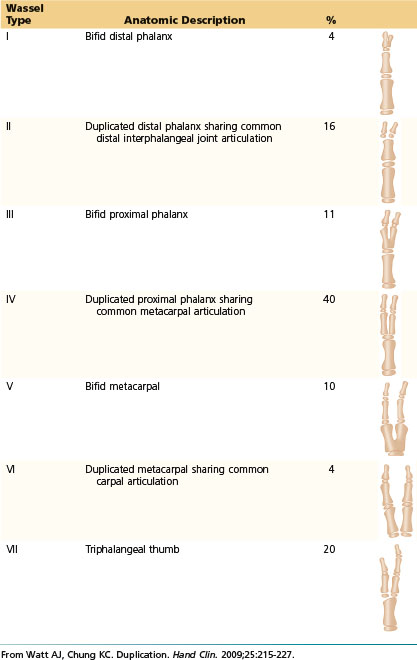
 The classification of duplicated thumb is based on the level of duplication, which ranges from type I, which is partial split of the distal phalanx, to type VII, which is complete split of the metacarpal (Table 37-1). The type corresponds to the number of abnormal skeletal elements present. For example, type III has three abnormal bones (two distal phalanges and a partially split proximal phalanx). Wassel type IV is the most common type (Fig. 37-1).
The classification of duplicated thumb is based on the level of duplication, which ranges from type I, which is partial split of the distal phalanx, to type VII, which is complete split of the metacarpal (Table 37-1). The type corresponds to the number of abnormal skeletal elements present. For example, type III has three abnormal bones (two distal phalanges and a partially split proximal phalanx). Wassel type IV is the most common type (Fig. 37-1).


Table 37-1 Classification of Thumb Duplication




Surgical Anatomy
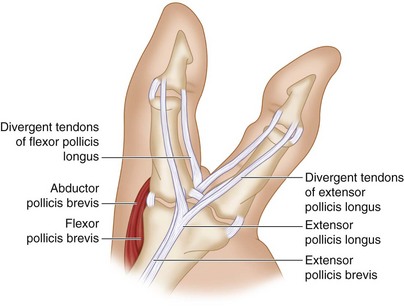
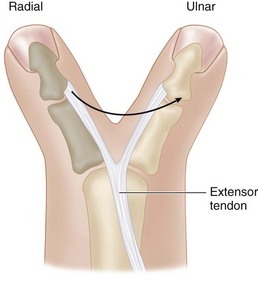
 The flexor and extensor tendons are split and insert eccentrically. An abnormal connection between the flexor and extensor tendons on the radial aspect of the thumb often exists as well. The origins and insertions of the thenar musculature, particularly the opponens pollicis (OP), are aberrant in cases of proximal duplication. The abductor pollicis brevis (APB) and flexor pollicis brevis (FPB) insert into the proximal phalanx of the radial duplicate, whereas the OP inserts into the radial metacarpal. The net effect of the long flexor tendons is to pull the distal phalanges into convergence while the thenar insertions create divergence at the proximal phalangeal level, creating a zigzag deformity (Fig. 37-3).
The flexor and extensor tendons are split and insert eccentrically. An abnormal connection between the flexor and extensor tendons on the radial aspect of the thumb often exists as well. The origins and insertions of the thenar musculature, particularly the opponens pollicis (OP), are aberrant in cases of proximal duplication. The abductor pollicis brevis (APB) and flexor pollicis brevis (FPB) insert into the proximal phalanx of the radial duplicate, whereas the OP inserts into the radial metacarpal. The net effect of the long flexor tendons is to pull the distal phalanges into convergence while the thenar insertions create divergence at the proximal phalangeal level, creating a zigzag deformity (Fig. 37-3).


Positioning


Exposures
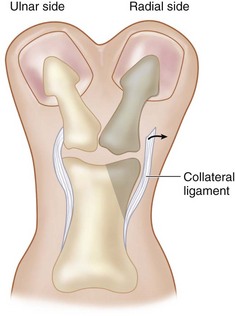
 When removing the radial thumb, one must retain a periosteal flap from the radial collateral ligament of the resected thumb to reconstruct the radial collateral ligament of the retained thumb. The extensor tendon from the resected thumb can be transferred to the ulnar side of the retained thumb for tendon.
When removing the radial thumb, one must retain a periosteal flap from the radial collateral ligament of the resected thumb to reconstruct the radial collateral ligament of the retained thumb. The extensor tendon from the resected thumb can be transferred to the ulnar side of the retained thumb for tendon.
 We describe the reconstruction of a type III and type IV thumb duplication.
We describe the reconstruction of a type III and type IV thumb duplication.
Pearls
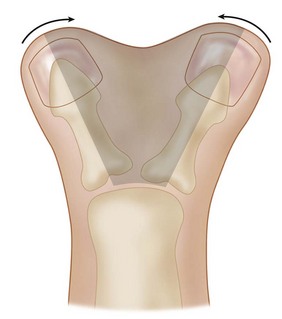
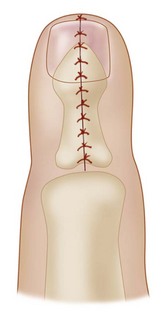
The Bilhaut-Cloquet procedure attempts to combine both thumbs into a single unit by removing the central portion of both thumbs to create a single thumb (Figs. 37-4 and 37-5). While conceptually appealing, it is exceedingly difficult to create an aesthetically pleasing thumb. A mismatch of the nail fold is common, and the cleft in the central combined thumb can be noticeable. It is preferable to accept a smaller thumb and use the soft tissue from the resected thumb to augment the size of the retained one.
Procedure
Reconstruction of a Type III Thumb Duplication
Step 1







Step 3


Step 5






Procedure
Reconstruction of Type IV Thumb Duplication
Step 1
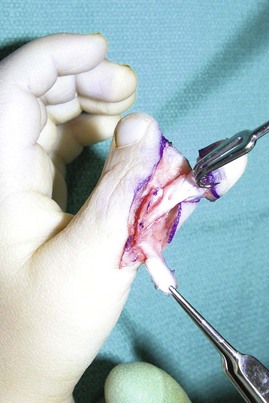
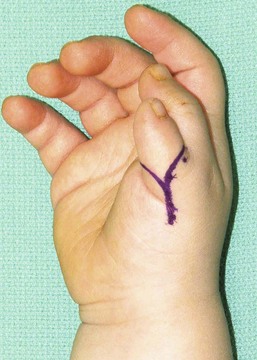
 The radial digit is selected for removal, and the skin incisions are designed as described previously (Figs. 37-15 and 37-16). The skin flaps are elevated sharply to expose the radial aspect of the metacarpophalangeal joint.
The radial digit is selected for removal, and the skin incisions are designed as described previously (Figs. 37-15 and 37-16). The skin flaps are elevated sharply to expose the radial aspect of the metacarpophalangeal joint.
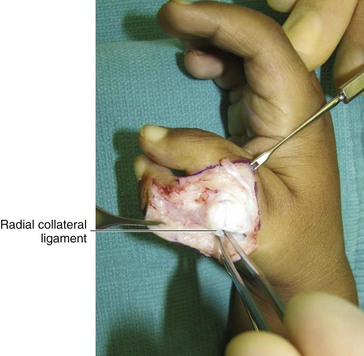
 The insertion of the APB is detached, and the radial collateral ligament is elevated off the base of the radial duplicate on a longitudinal periosteal flap (Fig. 37-17).
The insertion of the APB is detached, and the radial collateral ligament is elevated off the base of the radial duplicate on a longitudinal periosteal flap (Fig. 37-17).


Step 2


Step 3
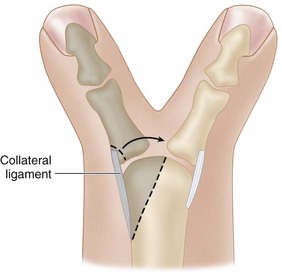
 A partial osteotomy of the radial portion of the head of the metacarpal is done to reduce its prominence. This osteotomy is easily performed using the knife blade with a back-and-forth motion over the unossified metacarpal (Figs. 37-19 and 37-20). Care should be taken to preserve the origin of the radial collateral ligament during this osteotomy.
A partial osteotomy of the radial portion of the head of the metacarpal is done to reduce its prominence. This osteotomy is easily performed using the knife blade with a back-and-forth motion over the unossified metacarpal (Figs. 37-19 and 37-20). Care should be taken to preserve the origin of the radial collateral ligament during this osteotomy.

Step 4


Step 5
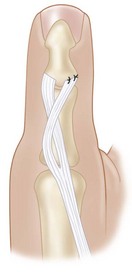
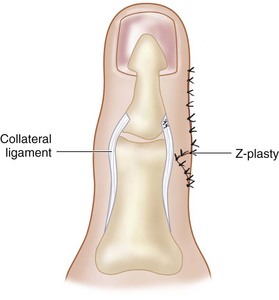
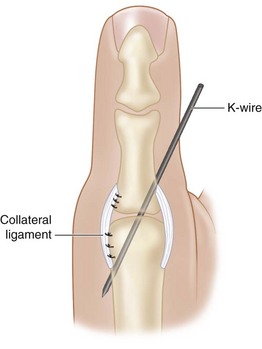
 The periosteal flap carrying the radial collateral ligament and the APB insertion is sutured to the radial base of the proximal phalanx using nonabsorbable braided suture. Additional sutures may be needed to reinfoirce the origin of the radial collateral liagment at the head of the metacarpal (Fig. 37-22).
The periosteal flap carrying the radial collateral ligament and the APB insertion is sutured to the radial base of the proximal phalanx using nonabsorbable braided suture. Additional sutures may be needed to reinfoirce the origin of the radial collateral liagment at the head of the metacarpal (Fig. 37-22).






Baek GH, Gong HS, Chung MS, et al. Modified Bilhaut-Cloquet procedure for Wassel type-II and III polydactyly of the thumb: surgical technique. J Bone Joint Surg [Am]. 2008;90:74-86.
Goldfarb CA, Patterson JM, Maender A, Manske PR. Thumb size and appearance following reconstruction of radial polydactyly. J Hand Surg [Am]. 2008;33:1348-1353.
Horii E, Hattori T, Koh S, Majima M. Reconstruction for Wassel type III radial polydactyly with two digits equal in size. J Hand Surg [Am]. 2009;34:1802-1807.
Ogino T, Ishii S, Takahata S, Kato H. Long-term results of surgical treatment of thumb polydactyly. J Hand Surg [Am]. 1996;21:478-486.



