Published on 02/03/2015 by admin
Filed under Internal Medicine
Last modified 22/04/2025
This article have been viewed 1224 times
Case 35
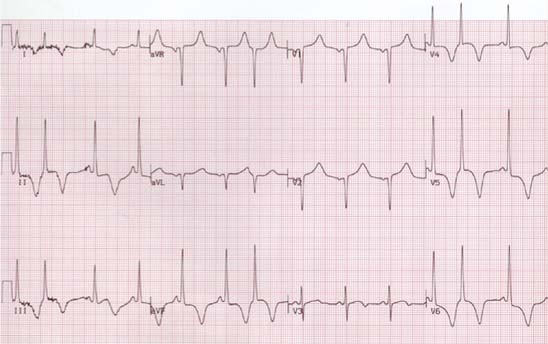
A 53-year-old African American male was admitted to the hospital with complaints of shortness of breath and dizziness. He was diagnosed with hypertension 4 to 5 years earlier and is receiving treatment. He also has hyperlipidemia and remote history of smoking. He has history of palpitations since childhood. There is family history of sudden death. His one brother died suddenly at age 43 years. ECG showed normal sinus rhythm with marked left ventricular hypertrophy, generalized ST-segment depression, and deep T-wave inversions in precordial as well as limb leads. His ECG is shown next. What is your interpretation?
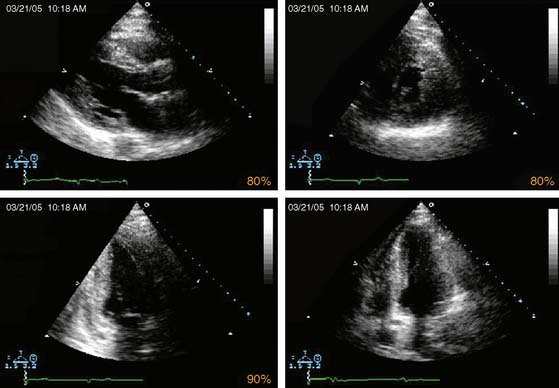
(Video 1)
Echo shows severe left ventricular hypertrophy (LVH). Left ventricular ejection fraction (LVEF) is 65% to 70%, without evidence of regional wall-motion abnormalities.
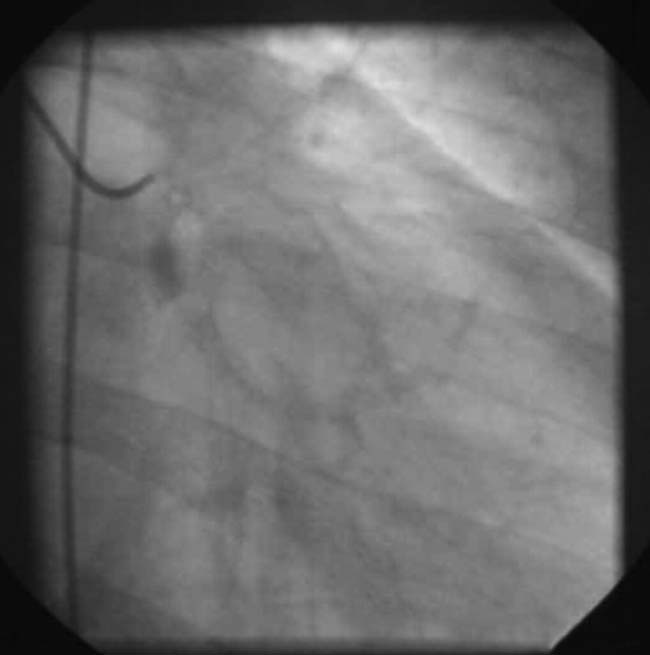
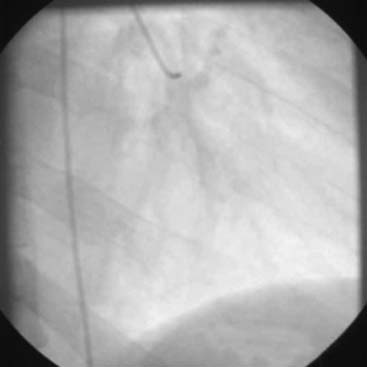
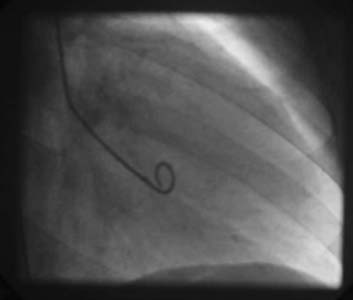
He was ruled out for acute myocardial infarction, but because of a very abnormal echocardiogram, he underwent cardiac catheterization and coronary angiography. This is shown next.
(Video 2)
(Video 3)
(Video 4)
Coronary arteries are normal with no luminal obstruction. LV cavity is small, and the LV is hyperdynamic, with cavity obliteration in the distal part of the LV during systole.
He was referred for exercise perfusion imaging to detect any exercise-induced arrhythmias and exercise-induced perfusion abnormalities. He was receiving verapamil.
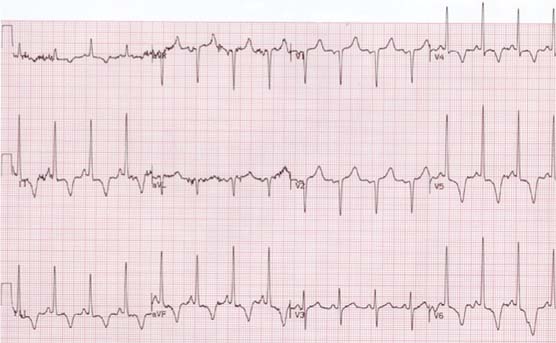
He underwent symptom-limited treadmill exercise using modified Bruce Protocol. He exercised for only 8:09 minutes, achieving an estimated workload of 4 METs. His heart rate increased from 80 to 98 beats/min and blood pressure from 100/70 to 120/80 mm Hg. He complained of tiredness and fatigue on exercise. His resting and peak exercise ECGs show is normal sinus rhythm with occasional premature ventricular beats. There is marked LVH with generalized ST-segment depression and deep symmetric T-wave inversion, and prolonged QTc. There is no arrhythmia with exercise. There is no change in ST-T with exercise. QT narrows with exercise, but QTc remains prolonged. There is alternans of T waves on the ECG.
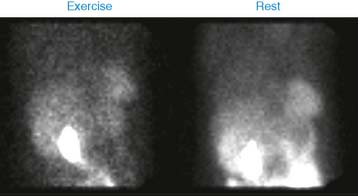
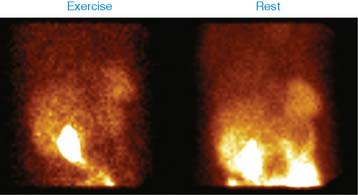
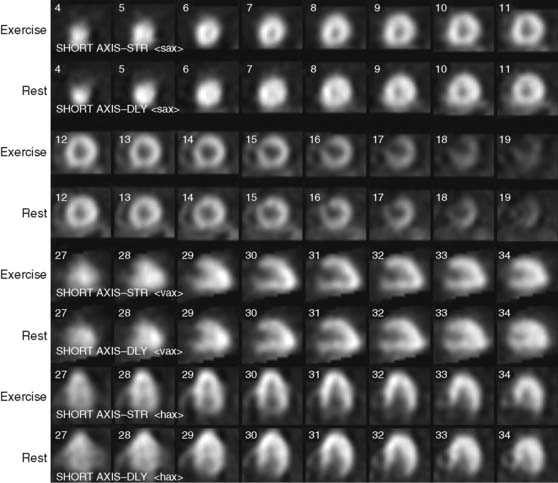
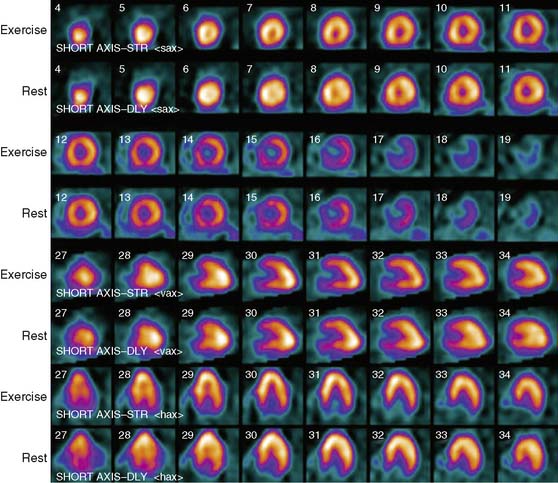
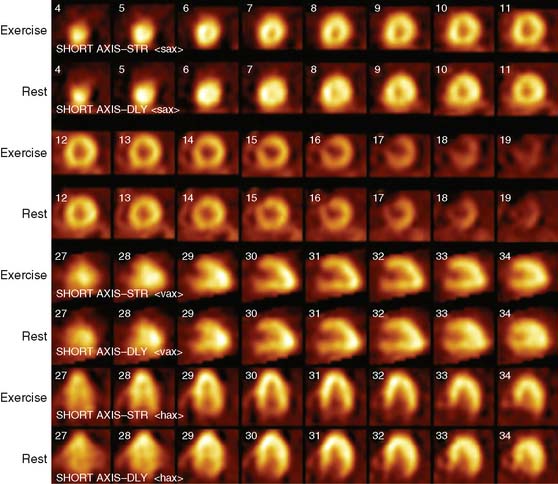
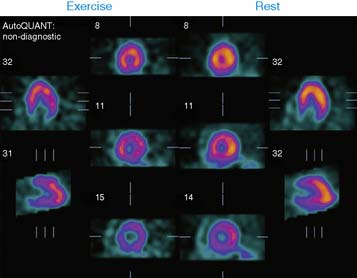
His stress and rest images are shown next. What is your interpretation?
(Fig. 1a)
(Fig. 1b)
(Video 5a)
(Video 5b)
(Fig. 2a)
(Fig. 2b)
(Fig. 2c)
(Fig. 6a)
(Fig. 6b)
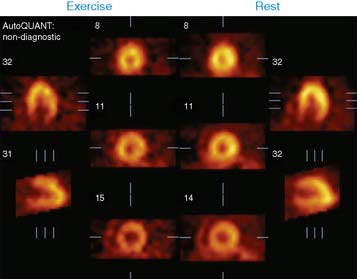
There is marked LVH with small left ventricular cavity. The hypertrophy appears to be more pronounced in the apical part of the LV. There is no regional perfusion abnormality. Interestingly, one can notice that the LV cavity is slightly bigger on the poststress images compared to the rest images. TID ratio was calculated at 1.24. The calculated LVEF is 31% on the poststress images and 36% on the rest images.
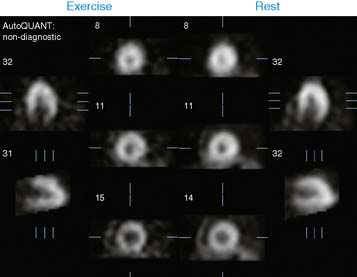
This case highlights the difficulties in calculation of LVEF by the automated gated SPECT programs. Generally, there is underestimation of the LVEF by these programs in hypertrophied ventricles secondary to the difficulties in reliably tracking the contours of the LV myocardium. These programs tend to assume only fixed thickness of the myocardium, as shown in the next images where LV contour is tracked by the myocardium. This results in underestimation of the LVEF.
This case also highlights another interesting phenomenon. Generally, transient dilation of the LV on the poststress images has been shown to be an indicator of severe multivessel coronary artery disease. However, it appears to be somewhat less specific in patients with LVH.
This patient has marked LVH, with normal coronary arteries and normal myocardial perfusion and function. Although the patient does have longstanding hypertension, the degree of LVH is disproportionate to what could be attributed to hypertensive heart disease. This raises the issue of hypertrophic cardiomyopathy, but in the absence of localized areas of hypertrophy in the LV, it is quite difficult to diagnose this condition.
In view of the history of dizziness, family history of sudden cardiac death, prolonged QTc, and T-wave alternans on the resting ECG, he underwent cardioverter-defibrillator (ICD) implantation.
Clinical Nuclear Cardiology State of the Art and Future Directio
WhatsApp us