[level-membership-for-allergy-and-immunology-category]
CASE 35
CW is a 30-year-old woman in your practice whose recent annual “Pap” smear results have just come to your attention. The diagnosis reads CIN type II (CIN = cervical intraepithelial neoplasia), which indicates inflammatory change and abnormal preneoplastic cells. You arrange a biopsy for her with your referring gynecologist, who confirms this result. In the meantime you order a serologic study for measurement of human papillomavirus 16 (HPV-16) antibody titers and a cervicovaginal lavage specimen to test for the presence of HPV-16 DNA. HPV-16 is implicated as a causative agent in cervical cancer. Based on recent findings in the literature, you wonder whether this woman could be considered for HPV-16 immunization. What other recommendations should you make?
QUESTIONS FOR GROUP DISCUSSION
RECOMMENDED APPROACH
Implications/Analysis of Laboratory Investigation
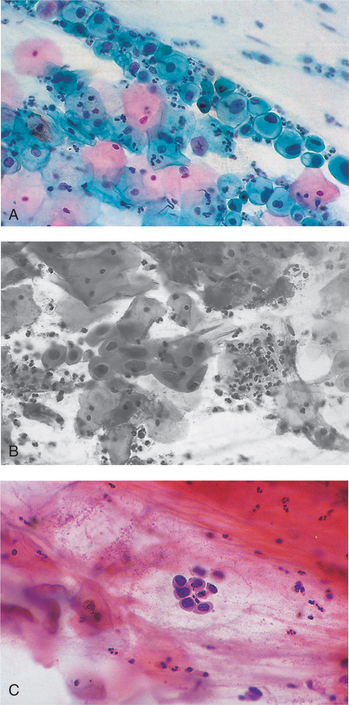
A Pap smear is a cytologic test performed on a sample of cells from the uterine cervix. This is a screening test to identify patients with premalignant lesions/cellular changes that could progress to malignancy. The quality of the specimen obtained and degree of accuracy with which the cytology is interpreted play a key role in correct diagnosis. When abnormal cells are identified on a Pap smear a colposcopy may be performed for a magnified look at the cervix (Fig. 35-1).
DIAGNOSIS
CW was diagnosed with HPV-16 infection as the likely cause of the CIN type II Pap smear result.
[/level-membership-for-allergy-and-immunology-category][not-level-membership-for-allergy-and-immunology-category]
CASE 35
CW is a 30-year-old woman in your practice whose recent annual “Pap” smear results have just come to your attention. The diagnosis reads CIN type II (CIN = cervical intraepithelial neoplasia), which indicates inflammatory change and abnormal preneoplastic cells. You arrange a biopsy for her with your referring gynecologist, who confirms this result. In the meantime you order a serologic study for measurement of human papillomavirus 16 (HPV-16) antibody titers and a cervicovaginal lavage specimen to test for the presence of HPV-16 DNA. HPV-16 is implicated as a causative agent in cervical cancer. Based on recent findings in the literature, you wonder whether this woman could be considered for HPV-16 immunization. What other recommendations should you make?
