CASE 35


History: A patient presents with chest pain.
1. What should be included in the differential diagnosis? (Choose all that apply.)
2. What is the most likely diagnosis?
3. What is the most common cause of left ventricular aneurysm?
A. Trauma
D. Tumor
4. On CT or MRI, what is the most reliable feature to distinguish a true aneurysm from a false aneurysm?
C. Location
ANSWERS
References
Walker CM, Reddy GP, Steiner RM. Radiology of the heart. In: Rosendorff C, ed. Essential Cardiology. ed 3 New York: Springer; 2013.
White RD. MR and CT assessment for ischemic cardiac disease. J Magn Reson Imaging. 2004;19(6):659–675.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 235–237.
Comment
Pathology and Etiology
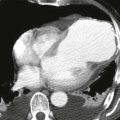
Left ventricular aneurysms result from transmural myocardial infarction. True aneurysms have focal wall thinning and akinesis, with bulging during systole. Most true aneurysms are located in the anteroapical region of the left ventricle and have wide necks. True aneurysms are usually managed medically. Surgical resection might be needed in the setting of poor ventricular function. A false aneurysm is actually a contained rupture. Most false aneurysms are inferoposterior in location and are connected to the left ventricle via a narrow neck. False aneurysms are usually treated surgically.
Imaging Findings and Diagnostic Criteria
Radiographs may show a contour abnormality along the left ventricle (Figs. A and B). Calcification may be present. With MRI or CT, true and false aneurysms can be differentiated on the basis of their ostia. A true aneurysm typically has an ostium that is greater than 50% of the aneurysm diameter, whereas a false aneurysm typically has an ostium that is less than 50% of the aneurysm diameter.