[level-membership-for-internal-medicine-category]
CASE 34 Left Main Dissection During Intervention
Cardiac catheterization
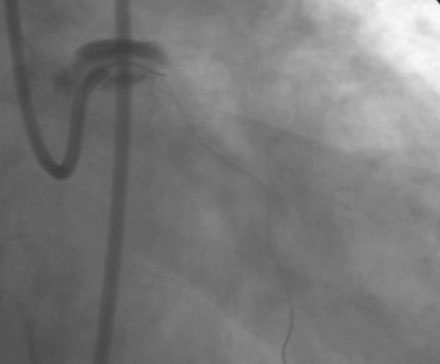
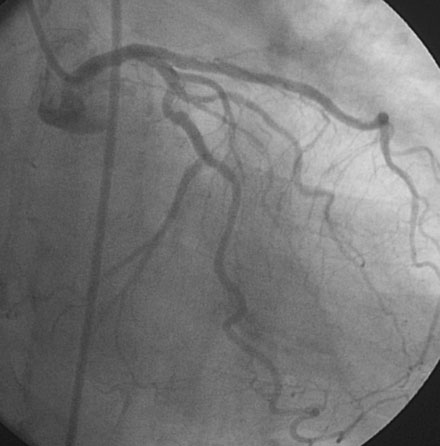
Coronary angiographic findings included moderate luminal narrowing in the right coronary artery, no significant obstructive disease of the left anterior descending artery, and severe disease in the circumflex involving the bifurcation of a large obtuse marginal branch (Figure 34-1 and Video 34-1). The operator anticipated difficulty with the proximal tortuosity of the circumflex and, after administration of bivalirudin, used an 8 French left Amplatz 2.0 guide catheter to engage the left coronary artery. Floppy-tipped guidewires were advanced into each branch of the circumflex and balloon angioplasty was performed (Figure 34-2). Following balloon angioplasty, angiography demonstrated persistent narrowing but no other angiographic complications (Video 34-2). The operator encountered difficulty advancing a 2.5 mm diameter by 18 mm sirolimus-eluting stent into the first obtuse marginal and achieved success by pushing the guide catheter deeply into the left main stem. After deploying the stent, angiography uncovered dissection of the left main stem (Figure 34-3 and Video 34-3). Several minutes after this angiogram, another coronary injection displayed dramatic worsening of the left main dissection (Figure 34-4 and Video 34-4) with near closure of the lumen and extensive contrast retention surrounding the left main stem. The patient reported severe chest pain but blood pressure and rhythm remained stable. A 3.5 mm diameter by 18 mm long sirolimus-eluting stent was deployed in the left main stem. This resolved her chest pain, restored luminal patency, and eliminated evidence of contrast retention (Figure 34-5 and Video 34-5).




Postprocedural course
She was readmitted 2 months later with atypical chest pain, and another coronary angiogram was performed that showed no significant obstructive disease. One year after the left main stent was placed, she again underwent angiography for recurrent atypical chest pain and an abnormal stress test. This again demonstrated wide patency of the left main and obtuse marginal stents (Figure 34-6 and Video 34-6).
Discussion
Coronary artery dissections occurring during percutaneous coronary intervention are most commonly caused by balloon barotrauma at the site of the lesion; however, dissection may also arise from the guidewire or, as shown in this case, from the guide catheter. Although this complication occurs uncommonly, guide catheter dissection can result in serious problems including abrupt vessel closure, extension into major proximal branches or the aorta, and a need for additional and unplanned stents.1 Several factors contribute to this complication, including the presence of ostial coronary disease, unusual vessel take-offs, and the use of aggressive guide catheters such as large bore (8 French or larger) or Amplatz catheters. The common practice of deep insertion of the guide catheter into the coronary artery in an effort to increase backup and allow passage of stents or balloons also leads to dissection, especially if the guide catheter is not coaxial to the artery. In the case shown here, left main dissection was likely caused by the large-bore Amplatz guide, chosen to support a circumflex intervention.
Management of a left main stem guide-related dissection depends on the extent of the dissection, its involvement with side branches or the aorta, and patient stability.1,2 Small dissections that do not retain contrast or impair the lumen can be treated conservatively and will usually heal without sequelae. Large dissections causing symptoms or luminal compromise need more definite treatment. Stent repair is often successful, but can be challenging if the dissection extends beyond the bifurcation of the left main into the left anterior descending artery and circumflex vessels. Similarly, dissection might cause abrupt closure of the left main and hemodynamic collapse, creating less than ideal conditions for performance of a complex intervention. Surgery is indicated if a large dissection cannot be repaired percutaneously.
1. Mulvihill N.T., Boccalatte M., Fajadet J., Marco J. Catheter-induced left main dissection: A treatment dilemma. Catheter Cardiovasc Interv. 2003;58:214-216.
2. Al-Saif S.M., Lie M.W., Al-Mubarak N., Agrawal S., Dean L.S. Percutaneous treatment of catheter-induced dissection of the left main coronary artery and adjacent aortic wall: A case report. Catheter Cardiovasc Interv. 2000;49:86-89.
[/level-membership-for-internal-medicine-category][not-level-membership-for-internal-medicine-category]
CASE 34 Left Main Dissection During Intervention
Cardiac catheterization
Coronary angiographic findings included moderate luminal narrowing in the right coronary artery, no significant obstructive disease of the left anterior descending artery, and severe disease in the circumflex involving the bifurcation of a large obtuse marginal branch (Figure 34-1 and Video 34-1). The operator anticipated difficulty with the proximal tortuosity of the circumflex and, after administration of bivalirudin, used an 8 French left Amplatz 2.0 guide catheter to engage the left coronary artery. Floppy-tipped guidewires were advanced into each branch of the circumflex and balloon angioplasty was performed (Figure 34-2). Following balloon angioplasty, angiography demonstrated persistent narrowing but no other angiographic complications (Video 34-2). The operator encountered difficulty advancing a 2.5 mm diameter by 18 mm sirolimus-eluting stent into the first obtuse marginal and achieved success by pushing the guide catheter deeply into the left main stem. After deploying the stent, angiography uncovered dissection of the left main stem (Figure 34-3 and Video 34-3). Several minutes after this angiogram, another coronary injection displayed dramatic worsening of the left main dissection (Figure 34-4 and Video 34-4) with near closure of the lumen and extensive contrast retention surrounding the left main stem. The patient reported severe chest pain but blood pressure and rhythm remained stable. A 3.5 mm diameter by 18 mm long sirolimus-eluting stent was deployed in the left main stem. This resolved her chest pain, restored luminal patency, and eliminated evidence of contrast retention (Figure 34-5 and Video 34-5).
