[level-membership-for-anesthesiology-category]
CHAPTER 34 Heart Failure
3 Describe the classification of heart failure




4 How is the severity of heart failure classified?




5 What major alterations in the heart occur in patients with heart failure?

where P = intracavity pressure, R = the radius of the chamber, and h = the thickness of the chamber wall.
7 How is cardiac output calculated? What is a normal cardiac output and index?

where CO = arterial pressure/ total peripheral resistance, SV = stroke volume and HR = heart rate.
9 What is systolic dysfunction?
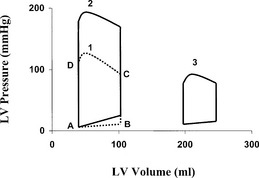
Systolic dysfunction leads to decreased ejection of blood from the left ventricle. The EF is diminished, the end-systolic and end-diastolic volume are enlarged, and the left ventricle is dilated. The stroke volume can be normal, but it is generated by a dilated ventricle with higher wall tension and oxygen consumption. In this pathologic condition the left ventricle has less reserve capacity to overcome pressure or volume load, which manifests in decreased exercise capacity (Figure 34-1, Loop 3).
10 What is diastolic dysfunction?
Diastolic dysfunction can occur with normal LV EF in many patients. Impaired LV relaxation or compliance or both are the major characteristic features of LV diastolic dysfunction. Early diastolic filling depends on the rapidity of ventricular relaxation, characterized by an energy-dependent reuptake of calcium from the cytosol into the sarcoplasmic reticulum of the myocytes. Late diastolic filling (atrial contraction) depends on LV compliance, which is the ratio of change in ventricular volume to change in ventricular diastolic pressure. In diastolic dysfunction the size of the LV cavity can be normal but ischemia, myocardial hypertrophy, pericardial constriction, fibrosis, or myocardial diseases alter the diastolic filling process. Systolic dysfunction with dilated left ventricle and high LV end-diastolic pressure accompanies significant diastolic dysfunction because of decreased LV relaxation and compliance (see Figure 34-1, Loop 2).
13 What physical signs suggest heart failure?
Key Points: Heart Failure
15 What treatment strategies are used in the different stages of heart failure?





16 What should be considered in preparing to conduct an anesthetic on patients with heart failure?




1. Crawford M.H. Current Diagnosis and Treatment in Cardiology, ed 2. New York: McGraw-Hill, 2003.
2. Fleisher L.A. Anesthesia and Uncommon Diseases, ed 5. Philadelphia: Saunders, 2006.
3. Fleisher L.A., Beckman J.A., Brown K.A., et al. ACC/AHA Guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: Executive summary. Circulation. 2007;116:1971-1996.
4. Hunt S.A., Abraham W.T., Chin M.H., et al. ACC/AHA Guideline update for the diagnosis and management of chronic heart failure in the adult: Task force on practice guidelines. Circulation. 2005;112:e154-e235.
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
CHAPTER 34 Heart Failure
3 Describe the classification of heart failure
4 How is the severity of heart failure classified?
5 What major alterations in the heart occur in patients with heart failure?
where P = intracavity pressure, R = the radius of the chamber, and h = the thickness of the chamber wall.
7 How is cardiac output calculated? What is a normal cardiac output and index?
where CO = arterial pressure/ total peripheral resistance, SV = stroke volume and HR = heart rate.
[/not-level-membership-for-anesthesiology-category]
