CASE 34
History: A 93-year-old woman presents with painless jaundice.
1. Which of the following should be included in the differential diagnosis of the dominant imaging findings? (Choose all that apply.)
2. What is this condition called?
3. Which of these conditions is a known predisposing factor for a patient to develop cholangiocarcinoma?
A. Postviral hepatitis fibrosis
B. Recurrent bacterial infection
4. This tumor is known to appear in a range of forms. Which of these choices is not a recognized form?
ANSWERS
CASE 34
Bile Duct Malignant Stricture (Klatskin’s Tumor)
1. C, D, and E
2. C
3. D
4. C
References
Bloom CM, Langer B, Wilson SR. Role of US in the detection, characterization, and staging of cholangiocarcinoma. Radiographics. 1999;19:1199–1218.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 232.
Comment
Cholangiocarcinomas are adenomatous tumors that arise from the lining of the bile ducts. Because they can arise from any portion of the biliary system (even the tiniest branches in the liver), the appearance of cholangiocarcinomas can be quite variable. They most often form nontumorous strictures, which are malignant cells spreading down the walls of the bile duct in a scirrhous pattern. They can also form polypoid masses that project into the lumen of the ducts. In the liver parenchyma itself, cholangiocarcinomas are often identified as liver masses and are indistinguishable from other liver tumors. Patients in whom these growths arise in the extrahepatic bile ducts have the best prognosis.
Cholangiocarcinomas can produce jaundice or other symptoms before they spread to adjacent structures. Cholangiocarcinoma is often fatal because it invades adjacent critical structures in the region, such as the bile ducts and portal vein. Distant metastases are not common.
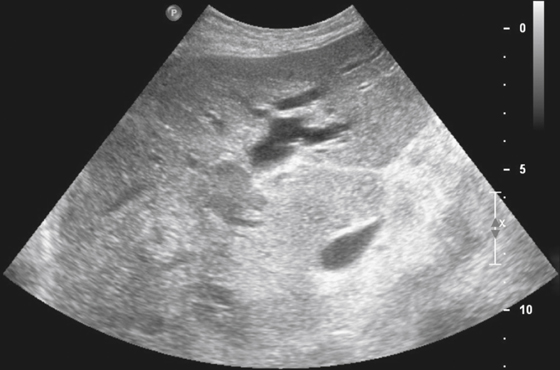
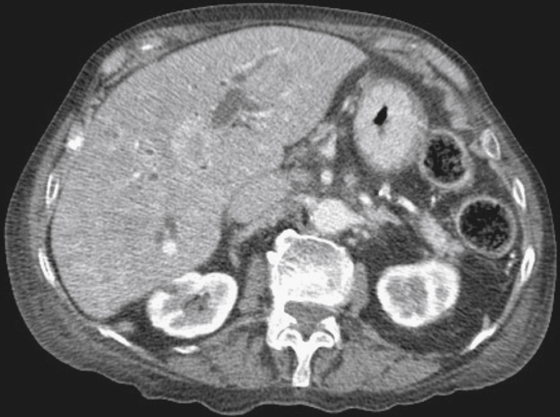
Ultrasound and CT inspection of the bile ducts reveals proximal ductal dilation (see figures), an area of narrowing, or a polypoid lesion in the duct lumen. Proximal ductal dilation is often evident. On CT examination, the tumors themselves are typically evident only when they are in the liver parenchyma and mass effect is visible. Approximately one third of cholangiocarcinomas manifest as liver masses because they grow exophytically into the liver parenchyma.
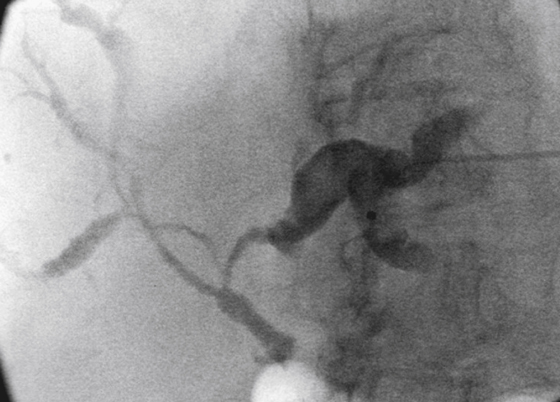
The type of cholangiocarcinoma that arises at the confluence of the right and left bile ducts is termed a Klatskin tumor. This tumor is typically scirrhous cholangiocarcinoma that grows along the ducts, producing thickening of the wall of the ducts and progressive narrowing of the lumen. As the tumor grows, focal lobar atrophy can become evident. CT can demonstrate a mass in the region. Direct cholangiography (either by percutaneous transhepatic cholangiography or by endoscopic retrograde cholangiopancreatography) demonstrates the extent and severity of biliary obstruction (see figures). The access achieved to the bile ducts also allows therapeutic maneuvers such as stenting to provide relief from jaundice. The condition is almost invariably fatal within 6 to 8 months because critical structures in the region, such as the portal vein, are often invaded. Enlarged lymph nodes in the porta hepatis and Mirizzi syndrome caused by an impacted stone in the cystic duct can mimic this condition.






