Case 34
Case 34
A 75-year-old male with hypertension, hyperlipidemia, and old myocardial infarction (26 years earlier) presented with complaints of occasional exertional angina. He never underwent cardiac catheterization, and he was treated medically.
Medications: lisinopril, isosorbide dinitrate, atorvastatin, and aspirin.
He was referred for exercise-rest myocardial perfusion imaging study.
He underwent symptom-limited treadmill exercise using Bruce Protocol. He exercised for 6:30 minutes, achieving an estimated workload of 7 METs. His heart rate increased from 75 to 144 beats/min, and blood pressure increased from 116/64 to 130/60 mm Hg. He developed no chest pain on exercise.
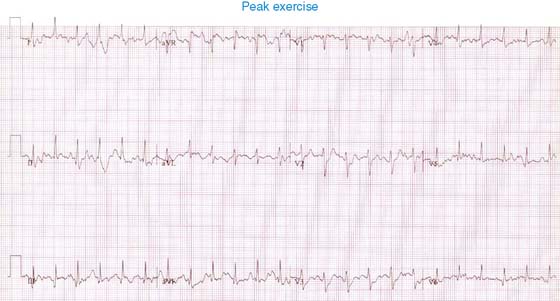
The test was terminated due to shortness of breath and fatigue. Baseline electrocardiogram shows normal sinus rhythm and Q waves in inferior and lateral leads, with no further ST-segment change on exercise.
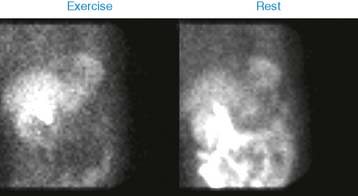
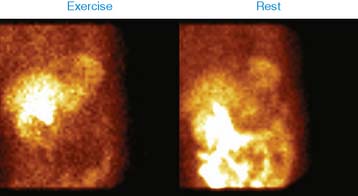
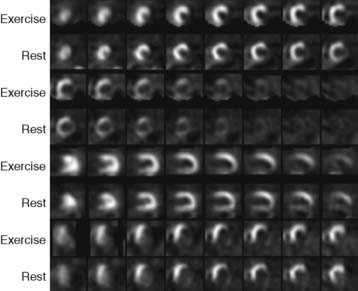
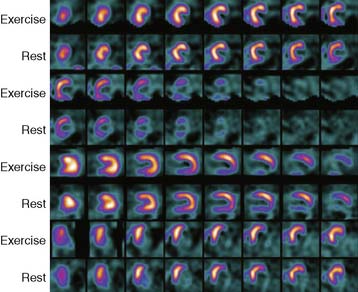
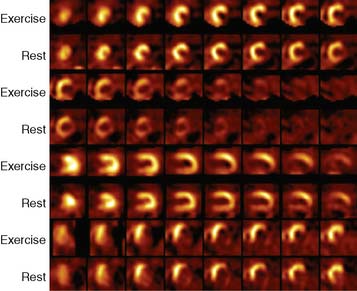
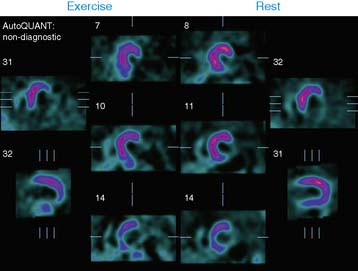
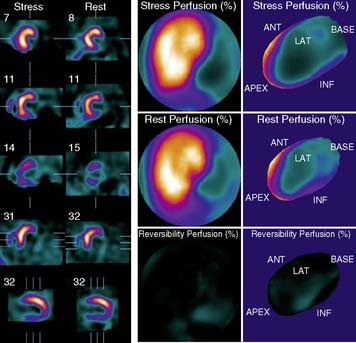
Exercise-rest perfusion imaging study shows a very large area of perfusion abnormality involving the inferior wall, lateral wall, and apex, with minimal reversibility in the inferior wall. The lateral wall is akinetic, and left ventricular ejection fraction is 34%.
Based upon the presence of a large scar involving the inferior and lateral wall, with only minimal ischemia involving the inferior wall, medical management was continued in this patient. No coronary angiography was performed in this case.
Clinical Nuclear Cardiology State of the Art and Future Directio