[level-membership-for-surgery-category]
Procedure 33 Correction of Swan-Neck Deformity in the Rheumatoid Hand
 See Video 25: Lateral Band Release for Rheumatoid Swan-Neck Deformity
See Video 25: Lateral Band Release for Rheumatoid Swan-Neck Deformity
Indications






Examination/Imaging
Clinical Examination
 Active and passive range of motion of the PIP joint is tested with the MCP joint in extension and flexion. This is to evaluate whether the intrinsic muscles are contributing to the restricted PIP joint motion. Restriction in radial and ulnar deviation is also tested with the MCP joint in extension to evaluate which of the intrinsic muscles is responsible for the PIP joint tightness.
Active and passive range of motion of the PIP joint is tested with the MCP joint in extension and flexion. This is to evaluate whether the intrinsic muscles are contributing to the restricted PIP joint motion. Restriction in radial and ulnar deviation is also tested with the MCP joint in extension to evaluate which of the intrinsic muscles is responsible for the PIP joint tightness.

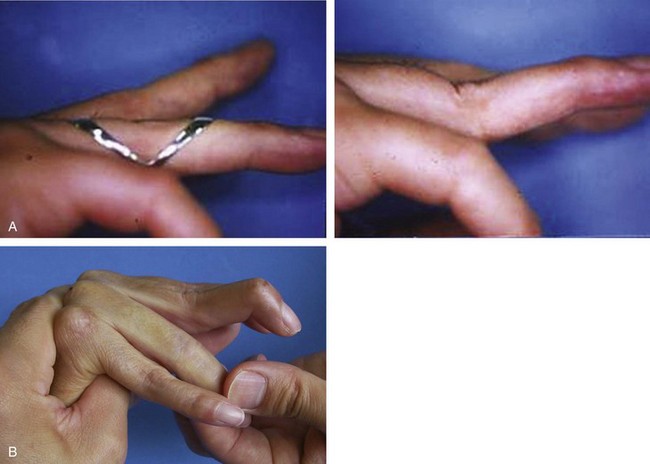
 When the PIP joint is flexible regardless of the metacarpophalangeal (MCP) joint position (type I), a PIP extension block splint may correct the deformity while restoring full flexion (Fig. 33-1A).
When the PIP joint is flexible regardless of the metacarpophalangeal (MCP) joint position (type I), a PIP extension block splint may correct the deformity while restoring full flexion (Fig. 33-1A).

 When passive flexion of the PIP is limited with the MCP joint in flexion, the pathology is the stiff PIP joint (type III) (Fig. 33-1B).
When passive flexion of the PIP is limited with the MCP joint in flexion, the pathology is the stiff PIP joint (type III) (Fig. 33-1B).
 The typical swan-neck deformity is associated with flexion contracture of the MCP joint, hyperextension of the PIP joints, and dorsally displaced lateral bands (Fig. 33-2).
The typical swan-neck deformity is associated with flexion contracture of the MCP joint, hyperextension of the PIP joints, and dorsally displaced lateral bands (Fig. 33-2).

Surgical Anatomy






Procedures to Prevent Hyperextension of the PIP Joint (for Types 1 to 3)
Bone Anchor Repair of the Volar Plate


Step 2
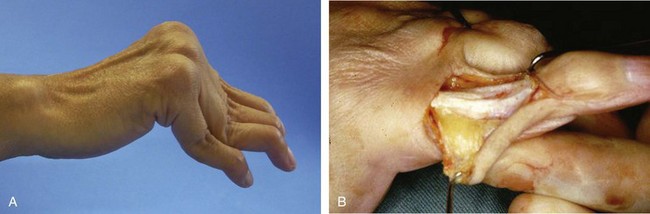
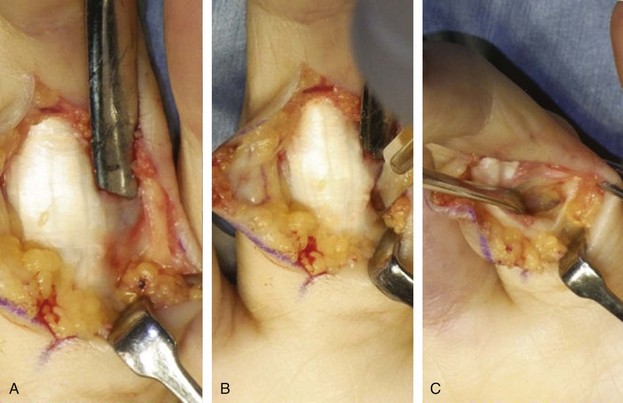
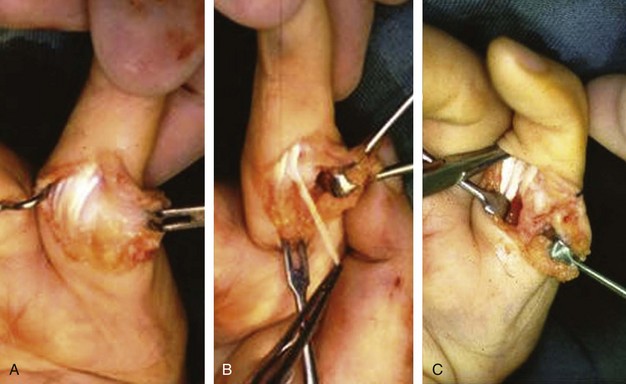
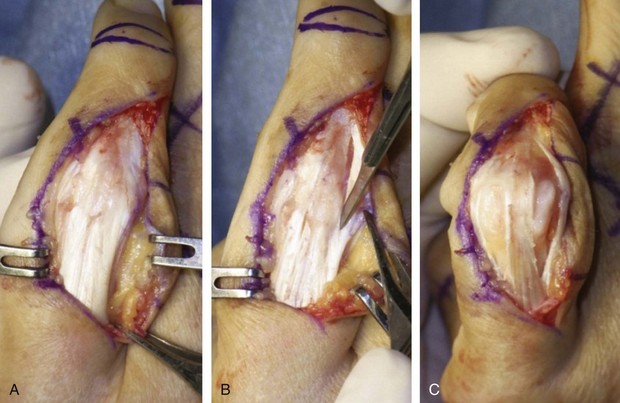
 The accessory collateral ligament is identified and incised (Fig. 33-5A and B). The volar plate with the entire flexor sheath is retracted laterally to expose the head of the proximal phalanx (Fig. 33-5C).
The accessory collateral ligament is identified and incised (Fig. 33-5A and B). The volar plate with the entire flexor sheath is retracted laterally to expose the head of the proximal phalanx (Fig. 33-5C).
Step 3


Step 4
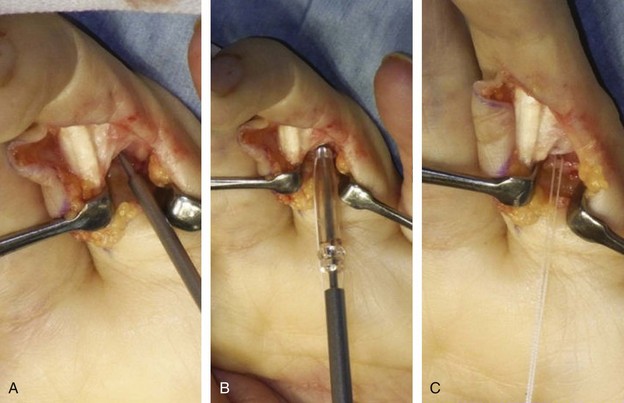
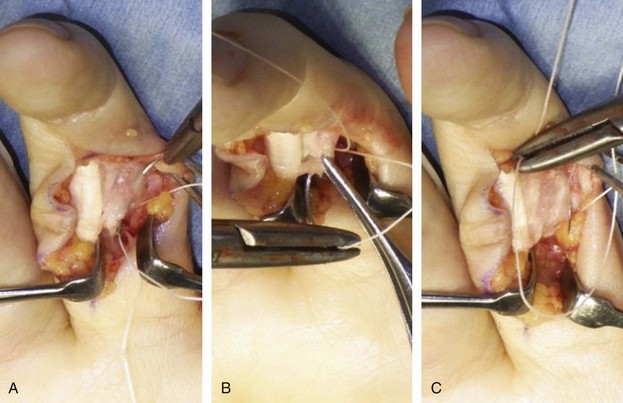
 The bone anchor typically has two needles with sutures. One needle is passed from the dorsolateral aspect of the volar plate (Fig. 33-7A) to emerge at the central portion of the volar plate (Fig. 33-7B). It is then passed through the edge of the previously divided accessory collateral ligament (Fig. 33-7C).
The bone anchor typically has two needles with sutures. One needle is passed from the dorsolateral aspect of the volar plate (Fig. 33-7A) to emerge at the central portion of the volar plate (Fig. 33-7B). It is then passed through the edge of the previously divided accessory collateral ligament (Fig. 33-7C).
Step 5
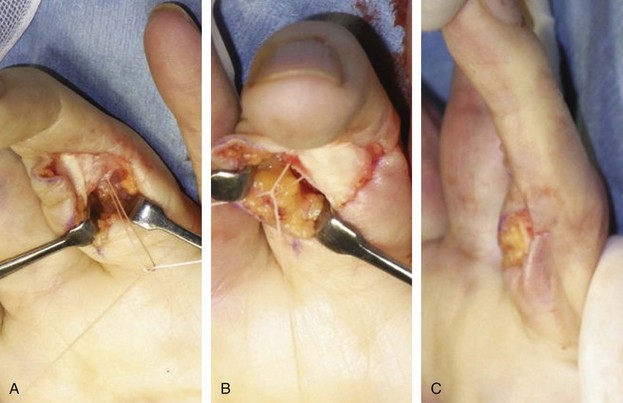
 The sutures are tied to each other, aiming to maintain the PIP joint in about 10 degrees of flexion (Fig. 33-8A).
The sutures are tied to each other, aiming to maintain the PIP joint in about 10 degrees of flexion (Fig. 33-8A).
 The other needle is passed in a similar fashion on the other side. After the second suture is tied, the PIP joint should be positioned in about 15 to 20 degrees of flexion. The first suture loop needs to shift medially to develop sufficient tension in the second suture loop (Fig. 33-8B and C).
The other needle is passed in a similar fashion on the other side. After the second suture is tied, the PIP joint should be positioned in about 15 to 20 degrees of flexion. The first suture loop needs to shift medially to develop sufficient tension in the second suture loop (Fig. 33-8B and C).
FDS Tenodesis


Retinacular Ligament Reconstruction

Step 2
 The divided lateral band is dissected distally and passed below the Cleland ligament so that the ulnar lateral band is now volar to the axis to the PIP joint to maintain the PIP joint in flexion. The lateral band is sutured to the A2 pulley or into the bone of the proximal phalanx to maintain the PIP joint in 15 to 20 degrees of flexion (Fig. 33-10B and C).
The divided lateral band is dissected distally and passed below the Cleland ligament so that the ulnar lateral band is now volar to the axis to the PIP joint to maintain the PIP joint in flexion. The lateral band is sutured to the A2 pulley or into the bone of the proximal phalanx to maintain the PIP joint in 15 to 20 degrees of flexion (Fig. 33-10B and C).
Procedures to Correct DIP Joint Deformity (for Types 1 to 4)




Procedures to Correct a Stiff Swan-Neck Deformity (Type 3)
Lateral Band Mobilization
Step 1

Step 2


Step-Cut (Z) Lengthening of the Central Slip
Step 1
 A step-cut lengthening of the central slip should be considered if shortening of the central slip restricts PIP joint flexion after manipulation of the PIP joint and mobilization of the lateral bands has been attempted.
A step-cut lengthening of the central slip should be considered if shortening of the central slip restricts PIP joint flexion after manipulation of the PIP joint and mobilization of the lateral bands has been attempted.
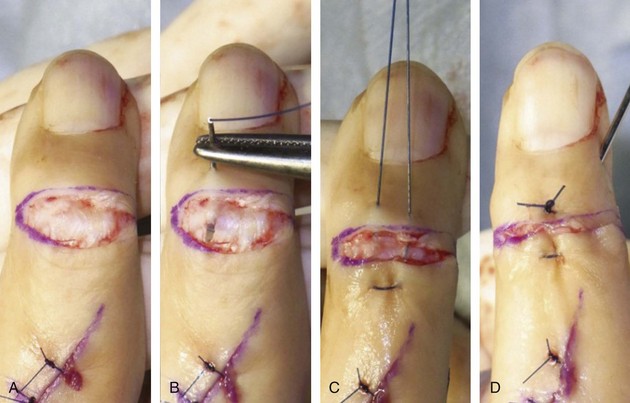
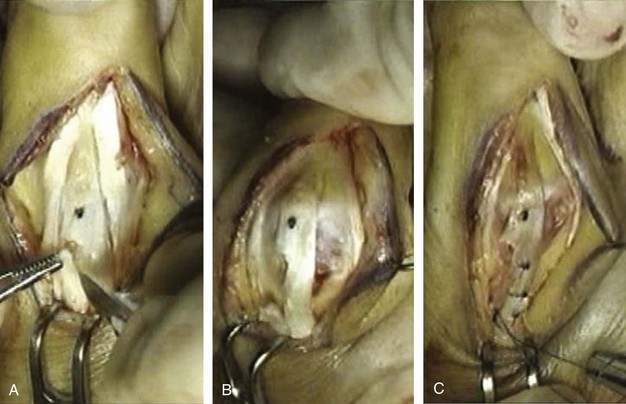
 A Z-incision of the central slip is made beginning 3 to 4 mm proximal to the insertion at the middle phalanx (marked as black dot on figures) and extended 1 to 1.5 cm proximally (depending on the severity of the deformity) (Fig. 33-13A).
A Z-incision of the central slip is made beginning 3 to 4 mm proximal to the insertion at the middle phalanx (marked as black dot on figures) and extended 1 to 1.5 cm proximally (depending on the severity of the deformity) (Fig. 33-13A).


Postoperative Care and Expected Outcomes
 Active motion should be encouraged as early as the second postoperative day.
Active motion should be encouraged as early as the second postoperative day.



 Figure 33-14 shows the appearance of the patient in Figure 33-2 one year after surgery. The patient underwent release of the ulnar intrinsic muscle, manipulation of the PIP joints, tenodermodesis of the DIP joint of the index and small fingers, and lateral band mobilization and volar plate reconstruction using bone anchors for the long and ring fingers. The swan-neck deformity was corrected, and all fingers had reasonable flexion except the small finger where the deformity recurred.
Figure 33-14 shows the appearance of the patient in Figure 33-2 one year after surgery. The patient underwent release of the ulnar intrinsic muscle, manipulation of the PIP joints, tenodermodesis of the DIP joint of the index and small fingers, and lateral band mobilization and volar plate reconstruction using bone anchors for the long and ring fingers. The swan-neck deformity was corrected, and all fingers had reasonable flexion except the small finger where the deformity recurred.
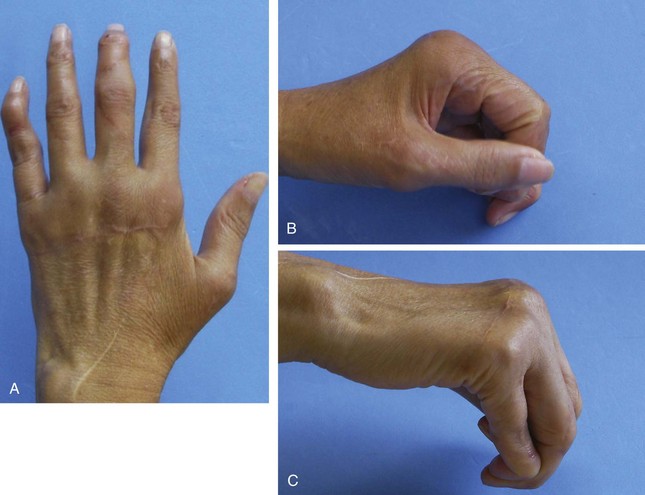
 Figure 33-15 shows a stiff swan-neck deformity with MP flexion-contractures of all fingers in a 49-year-old woman. She underwent intrinsic muscle release and lateral band mobilization of all fingers. In addition, lengthening of the central slip was done for the long and ring fingers. An extension block pin was inserted into the head of the proximal phalanx to protect the central slip repair, and the distal wounds were left open. Excellent flexion of the PIP joint in 6 months (Fig. 33-15C) and at the10-year follow-up showed that the correction of the deformity was maintained (Fig. 33-15D and 33-15E).
Figure 33-15 shows a stiff swan-neck deformity with MP flexion-contractures of all fingers in a 49-year-old woman. She underwent intrinsic muscle release and lateral band mobilization of all fingers. In addition, lengthening of the central slip was done for the long and ring fingers. An extension block pin was inserted into the head of the proximal phalanx to protect the central slip repair, and the distal wounds were left open. Excellent flexion of the PIP joint in 6 months (Fig. 33-15C) and at the10-year follow-up showed that the correction of the deformity was maintained (Fig. 33-15D and 33-15E).

de Bruin M, van Vliet DC, Smeulders MJ, Kreulen M. Long-term results of lateral band translocation for the correction of swan neck deformity in cerebral palsy. J Pediatr Orthop. 2010;30:67-70.
Kiefhaber TR, Stricland JW. Soft tissue reconstruction for rheumatoid swan-neck and boutonniere deformities: long term results. J Hand Surg [Am]. 1993;18:984-989.
Ozturk S, Zor F, Sengezar M, Isik S. Correction of bilateral congenital swan-neck deformity by use of Mitek mini anchor: a new technique. Br J Plast Surg. 2005;56:822-825.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
Procedure 33 Correction of Swan-Neck Deformity in the Rheumatoid Hand
See Video 25: Lateral Band Release for Rheumatoid Swan-Neck Deformity
Indications
Examination/Imaging
Clinical Examination
Active and passive range of motion of the PIP joint is tested with the MCP joint in extension and flexion. This is to evaluate whether the intrinsic muscles are contributing to the restricted PIP joint motion. Restriction in radial and ulnar deviation is also tested with the MCP joint in extension to evaluate which of the intrinsic muscles is responsible for the PIP joint tightness.
When the PIP joint is flexible regardless of the metacarpophalangeal (MCP) joint position (type I), a PIP extension block splint may correct the deformity while restoring full flexion (Fig. 33-1A).
When passive flexion of the PIP is limited with the MCP joint in flexion, the pathology is the stiff PIP joint (type III) (Fig. 33-1B).
The typical swan-neck deformity is associated with flexion contracture of the MCP joint, hyperextension of the PIP joints, and dorsally displaced lateral bands (Fig. 33-2).
Surgical Anatomy
Procedures to Prevent Hyperextension of the PIP Joint (for Types 1 to 3)
Bone Anchor Repair of the Volar Plate
Step 2
The accessory collateral ligament is identified and incised (Fig. 33-5A and B). The volar plate with the entire flexor sheath is retracted laterally to expose the head of the proximal phalanx (Fig. 33-5C
[/not-level-membership-for-surgery-category]
