CASE 31
RR, a 17-year-old woman who was previously well, has been admitted to the hospital because of fever, rash, generalized fatigue, and acute pain in the left eye. In the last 2 months she has lost 12 kg in weight and reports an intermittent fever with fatigue of the same duration. She has had multiple sexual partners and a therapeutic abortion at 14 years of age. There has been no recent travel, and a tuberculosis skin test is negative (with positive control). She appears ill, has marked conjunctival infection, a tender sclera with palpation, and left retinal detachment with some peri-orbital swelling. Fundoscopic/ophthalmoscopic examination (of the optic disc, blood vessels, and retina) is otherwise normal. The remainder of the ears, nose, and throat examination is unremarkable, although she does have prominent nontender cervical nodes. There is also swelling of the inguinal nodes, a macular rash (small, flat spots) on the thigh, and a faint cardiac murmur in the upper chest.
An HIV (ELISA) and a syphilis (VDRL) test were ordered immediately, as was a urine and blood screen culture, and chest radiograph. HIV tests were negative, but a serologic test for syphilis was positive, although a hemagglutination test for Treponema pallidum was negative (i.e., a “false positive” syphilis test was seen). Urine showed 2+ (30 mg/dL) protein, some red blood cells, and some hyaline casts (generally reflecting inflammatory changes in the upper urinary tract, including the kidney). Blood screen indicated that she was moderately anemic (hemoglobin 80% of normal; see Appendix for reference value), with a lymphopenia (lymphocyte counts about 20% of normal) and low platelets. The chest radiograph was normal. A bone marrow aspirate with smear was performed. However, there was no evidence for lymphoma or leukemia, Hodgkin’s disease, malignant histiocytosis (resident macrophages in connective tissue), or other immunolymphoproliferative disorders. Computed tomography (CT) showed swelling of the soft tissues around the left eye and evidence for cerebral atrophy. Blood cultures remained negative throughout hospitalization.
QUESTIONS FOR GROUP DISCUSSION
RECOMMENDED APPROACH
Implications/Analysis of Family History
No family history is provided. See Cases 18 and 22 for genetics of this disorder.
Implications/Analysis of Laboratory Investigation
Rheumatologic Disorders as Possibilities
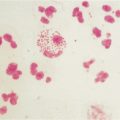
Vasculitis is an inflammation of the blood vessels that results from narrowing of the inflamed vessels and, hence, insufficient blood flow to the affected organ (Fig. 31-1). Therefore, manifestations or symptoms depend on the particular vessels involved. Polyarteritis nodosa, a multisystemic disease that often involves the skin, nerves, heart, gut, and kidneys might be considered except that most cases occur in 40- to 60-year-old patients. Dermatomyositis might be considered, bearing in mind the vague symptoms and the rash. Blood work to eliminate muscle inflammation essentially removes the latter from consideration.

Immune Complex Disorder
High on the list of possibilities is systemic lupus erythematosus (SLE). Immune complex deposition in different tissues would explain the results of the urinalysis, CT, and false-positive VDRL assay. As well, lymphopenia, thrombocytopenia, cardiac signs (the murmur referred to earlier), and the rash are consistent with a diagnosis of SLE. The rash results from blood leaking out of damaged blood vessels during the inflammatory processes. The cerebral atrophy is striking in one so young, but it could represent lupus cerebritis, an inflammation of the brain. Therefore, tests to determine the ANA and anti-DNA titer, as well as a biopsy of the rash were ordered (see Additional Laboratory Tests).
Additional Laboratory Tests
A serologic test for ANA was performed (positive at a titer of 1:2000). Antibodies to double-stranded DNA were detected at high titer (1:640), and complement C3 and C4 were low, as were total serum complement levels (see Case 11). Biopsy of the rash showed features typical of leukocytoclastic (small vessel) vasculitis.
Aminoff M, et al. Mutations in CUBN, encoding the intrinsic factor-vitamin B12 receptor, cubilin, causes hereditary megaloblastic anaemia 1. Nat Genet. 1999;21:309.
Andersen MS, et al. Projection of an immunological self shadow with the thymus by the AIRE protein. Science. 2002;298:1395.
Andres E, et al. Efficacy of short-term oral cobalamin therapy for the treatment of cobalamin deficiencies related to food-cobalamin malabsorption: A study of 30 patients. Clin Lab Haematol. 2003;25:161.
Ang CW, Jacobs BC, Laman JD. The Guillain-Barré syndrome: A true case of molecular mimicry. Trends Immunol. 2004;25:61.
Arbuckle MR, et al. Development of autoantibodies before clinical onset of systemic lupus erythematosus. N Engl J Med. 2003;349:1526.
Atkinson MA, Eisenbarth GS. Type 1 diabetes: New perspectives on disease pathogenesis and treatment. Lancet. 2001;358:221.
Au A, O’Day J. Review of severe vaso-occlusive retinopathy in systemic lupus erythematosus and the antiphospholipid syndrome: Associations, visual outcomes, complications and treatment. Clin Exp Ophthalmol. 2004;32:87.
Baudon JJ, et al. Diagnosing celiac disease: A comparison of human tissue transglutaminase antibodies with antigliadin and antiendomysium antibodies. Arch Pediatr Adolesc Med. 2004;158:584.
Bolaman Z, et al. Oral versus intramuscular cobalamin treatment in megaloblastic anemia: A single center, prospective, randomized, open-label study. Clin Ther. 2003;25:3124.
Brasington RD, et al. Immunologic rheumatic disorders. J Allergy Clin Immunol. 2003;111:S593.
Centers for Disease Control and Prevention. Lyme disease–United States, 2001-2002. JAMA. 2004;291:2810.
Cervera R, Asherson RA. Clinical and epidemiological aspects in the antiphospholipid syndrome. Immunobiology. 2003;207:5.
Ciccarelli O, Miller DH. Magnetic resonance imaging in multiple sclerosis. Practical Neurol. 2002;2:103.
Cohen SB, et al. Patient-versus physician-reported outcomes in rheumatoid arthritis patients treated with recombinant interleukin-1 receptor antagonist (anakinra) therapy. Rheumatology. 2004;43:704.
Cole P, Rabasseda X. The soluble tumor necrosis factor receptor etanercept: A new strategy for the treatment of autoimmune rheumatic disease. Drugs Today. 2004;40:281.
Csernok E. Anti-neutrophil cytoplasmic antibodies and pathogenesis of small vessel vasculitis. Autoimmun Rev. 2003;2:158.
Delarasse C, et al. Myelin/oligodendrocyte glycol-protein-deficient (MOG-deficient) mice reveal lack of immune tolerance to MOG in wild-type mice. J Clin Invest. 2003;112:544.
Devendra D, Eisenbarth GS. Immunologic endocrine disorders. J Allergy Clin Immunol. 2003;11:S624.
Devlin SM, Andrews CN, Beck PL. Celiac disease: CME update for family physicians. Can Fam Physician. 2004;50:719.
Eisenbarth GS, Gottlieb PA. Autoimmune polyendocrine syndromes. N Engl J Med. 2004;350:2068.
Ekerfelt C, et al. Lyme borreliosis in Sweden: Diagnostic performance of five commercial Borrelia serology kits using sera from well-defined patient groups. APMIS. 2004;112:74.
Fasano A, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: A large multicenter study. Arch Intern Med. 2003;163:286.
Finkel HE, et al. Blindness in a vegan. N Engl J Med. 2000;343:585.
Fletcher DD, et al. Long-term outcome in patients with Guillain-Barré syndrome requiring mechanical ventilation. Neurology. 2000;54:2311.
Fyfe JC, et al. The functional cobalamin (vitamin B12)-intrinsic factor receptor is a novel complex of cubilin and amnionless. Blood. 2004;103:1573.
Gill JM, et al. Diagnosis of systemic lupus erythematosus. Am Fam Physician. 2003;68:2179.
Gordon MM, et al. A genetic polymorphism in the coding region of the gastric intrinsic factor gene (GIF) is associated with congenital intrinsic factor deficiency. Hum Mutat. 2004;23:85.
Grimm D, et al. Outer-surface protein C of the Lyme disease spirochete: A protein induced in ticks for infection of mammals. Proc Natl Acad Sci U S A. 2004;101:3142.
Halonen M, et al. AIRE mutations and human leukocyte antigen genotypes as determinants of the autoimmune polyendo-crinopathy-candidiasis-ectodermal dystrophy phenotype. J Clin Endocrinol Metab. 2002;87:2568.
Harrison MJ, Ravdin LD. Cognitive dysfunction in neuropsychiatric system lupus erythematosus. Clin Opin Rheumatol. 2002;14:510.
Hayes EB, Piesman J. How can we prevent Lyme disease? N Engl J Med. 2003;348:2424.
Homo-Delarche F, Drexhage HA. Immune cells, pancreas development regeneration and type 1 diabetes. Trends Immunol. 2004;25:222.
Kang I, Park SH. Infectious complications in SLE after immunosuppressive therapies. Curr Opin Rheumatol. 2003;15:528.
Klein L, et al. Shaping of the autoreactive T-cell repertoire by a splice variant of self protein expressed in thymic epithelial cells. Nat Med. 2000;6:56.
Kroesen S, et al. Serious bacterial infections in patients with rheumatoid arthritis under TNF-α therapy. Rheumatology. 2003;42:617.
Lassmann H, Ransohoff RM. The CD4-Th1 model for multiple sclerosis: A crucial re-appraisal. Trends Immunol. 2004;25:275.
Londie M, Maiuri L. Gliadin as stimulator adaptive and innate immune responses in celiac disease. J Pediatr Gastroenterol Nutr. 2004;39:S729.
Martin S, et al. Development of type 1 diabetes despite severe hereditary B-cell deficiency. N Engl J Med. 2001;345:1036.
Muller WA. Leukocyte-endothelial-cell interactions in leukocyte transmigration and the inflammatory response. Trends Immunol. 2003;24:327.
Myhre AG, et al. Autoimmune adrenocortical failure in Norway autoantibodies and human leukocyte antigen Class II associations related to clinical features. J Clin Endocrinol Metab. 2002;87:618.
Nadelman RB, Wormser GP. Recognition and treatment of erythema migrans: Are we off target? Ann Intern Med. 2002;136:477.
Nyholm E, et al. Oral vitamin B12 can change our practice. Postgrad Med J. 2003;79:218.
Ochi K, et al. Changes in serum macrophage-related factors in patients with chronic inflammatory demyelinating polyneuropathy caused by intravenous immunoglobulin therapy. J Neurol Sci. 2003;208:43.
Oh R, Brown DL. Vitamin B12 deficiency. Am Fam Physician. 2003;67:979.
Ozbek S, et al. Delay in the diagnosis of SLE: The importance of arthritis/arthralgia as the initial symptom. Acta Med Okayama. 2003;57:187.
Pedotti R, et al. Multiple elements of the allergic arm of the immune response modulate autoimmune demyelination. Proc Natl Acad Sci U S A. 2003;100:1867.
Polman CH, Uitdehaag M. New and emerging treatment options for multiple sclerosis. Lancet Neurol. 2003;2:563.
Rossi T. Celiac disease. Adolesc Med Clin. 2004;15:91.
Seneviratne U. Guillain-Barré syndrome. Postgrad Med J. 2000;76:774.
Settles B, et al. Down regulation of cell adhesion molecules LFA-1 and ICAM-1 after in vitro treatment with anti-TNF-alpha agent thalidomide. Cell Mol Biol. 2001;47:1105.
Sollid LM, Gray GM. A role for bacteria in celiac disease? Am J Gastroenterol. 2004;99:905.
Steere AC, Coburn J, Glickstein L. The emergence of Lyme disease. J Clin Invest. 2004;113:1093.
Steere AC. Duration of antibiotic therapy for Lyme disease. Ann Intern Med. 2003;138:761.
Toh BH, van Driel IR, Gleeson PA. Pernicious anemia. N Engl J Med. 1997;337:1441.
Torrance GW, et al. Improvement in health utility among patients with rheumatoid arthritis treated with adalimumab (a human anti-TNF monoclonal antibody) plus methotrexate. Rheumatology. 2004;43:712.
Van Koningsveld R, et al. Effect of methylprednisolone when added to standard treatment with intravenous immunoglobulin for Guillain-Barré syndrome: Randomized trial. Lancet. 2004;363:192.
Van Rhijn I, et al. Gamma/delta T cell non-responsiveness in Campylobacter jejuni-associated Guillain-Barré syndrome patients. Neurology. 2003;61:994.
Wanschiz J, et al. Distinct time pattern of complement activation and cytotoxic T cell response in Guillain-Barré syndrome. Brain. 2003;126:2034.
Ward PC. Modern approaches to the investigation of vitamin B12 deficiency. Clin Lab Med. 2002;22:435.
Watson JA, Clearman B, Mitros F. Effect of a gluten-free diet on gastrointestinal symptoms in celiac disease. Am J Clin Nutr. 2004;79:669.
White S, Rosen A. Apoptosis in systemic lupus erythematosus. Curr Opin Rheumatol. 2003;15:557.
Widhe M, et al. Borrelia-specific interferon-gamma and interleukin-4 secretion in cerebrospinal fluid and blood during Lyme borreliosis in humans: Association with clinical outcome. J Infect Dis. 2004;189:1881.
Williams AJK, et al. The high prevalence of autoantibodies to tissue transglutaminases in first degree relatives of patients with type 1 diabetes is not associated with islet autoimmunity. Diabetes Care. 2001;24:504.
Yang XF, et al. Essential role of OSpA/B in the life cycle of the Lyme disease spirochete. J Exp Med. 2004;199:641.