CASE 31


1. What are etiologies for this appearance? (Choose all that apply.)
D. Syphilis
2. What is the most likely diagnosis?
D. Syphilis
3. Which of the following is not a complication of this condition?
A. Rupture
C. Dissection
4. Which MRI technique could be used to quantify aortic regurgitation?
A. Double inversion recovery (black blood)
ANSWERS
Reference
Reddy GP, Gunn M, Mitsumori LM, et al. Multislice CT and MRI of the thoracic aorta. In: Webb WR, Higgins CB, eds. Thoracic Imaging: Pulmonary and Cardiovascular Radiology. ed 2 Philadelphia: Lippincott Williams & Wilkins; 2010.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 388–389.
Comment
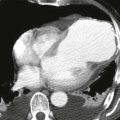
Pathology and Etiology
Enlargement of the aortic root and ascending aorta is characteristic of annuloaortic ectasia. The dilation of the aorta in this condition may stop at the sinotubular junction or extend to involve the entire ascending aorta, which is sometimes called the “tulip bulb” configuration. Annuloaortic ectasia results from cystic medial necrosis, which can be idiopathic or can be associated with Marfan syndrome or Ehlers-Danlos syndrome.
Complications
Complications of annuloaortic ectasia include aortic dissection, aortic rupture, and aortic regurgitation. Although 5.5–6 cm is the usual threshold of aortic diameter that necessitates surgery, operative repair may be indicated in annuloaortic ectasia when the aorta reaches a diameter of 5 cm owing to the high risk of rupture.