CASE 30

History: A 70-year-old man presents with epigastric pain and weight loss.
1. In what condition is the Carmen meniscus sign (CMS) found?
2. What is the Kirkland complex?
A. The central excavated collection of barium due to ulceration
B. The concave lucent margin around the ulceration
C. The distorted rugal folds around the ulceration
D. The mass effect surrounding the ulceration
3. Where must the lesion be located for the CMS to be seen?
A. The lesion may occur anywhere in the stomach
B. The lesion must occur on the lesser curvature of body or antrum
C. The lesion must obliterate the cardiac rosette at the gastroesophageal junction
D. The lesion must invade the pylorus, causing gastric outlet obstruction
4. How is the CMS best seen?
A. It is best seen with 3D ultrasonography
B. It is best seen with CT virtual gastrography
C. It is best seen on single-contrast or biphasic studies
D. It is best seen on double-contrast barium studies
ANSWERS
CASE 30
Carmen Meniscus Sign
1. C
2. B
3. B
4. C
Reference
Low VHS, Levine MS, Rubesin SE, et al: Diagnosis of gastric carcinoma: sensitivity of double-contrast barium studies. Am J Roentgenol. 1994;162:329–334.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 82-85.
Comment
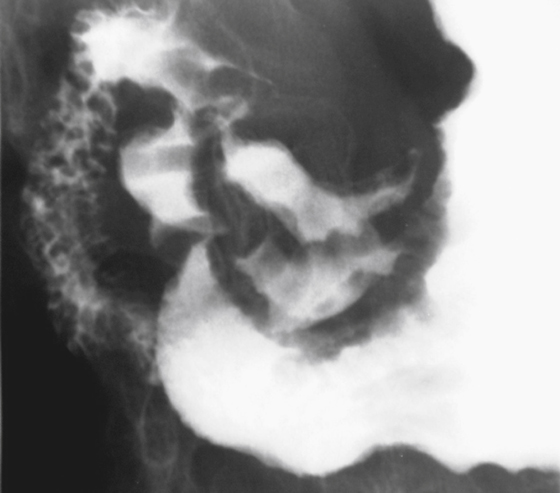
The Carmen meniscus sign was first described by Dr. Carmen in the late 1930s before double-contrast studies were in routine use. It is a sign that is considered to be pathognomic for an ulcerated gastric malignancy. The sign is confusing and not well understood. This is because certain conditions must be present for the sign to occur. First, the lesion must be a flat infiltrating ulcerative lesion with heaped-up margins. Second, the lesion must be in the saddle region of the stomach, the lesser curve of the body or antrum (see figures). The examination should be a single-contrast or at least a biphasic study (when both single-contrast and double-contrast evaluation are used). The sign may be seen on a double-contrast study but is often not recognized. Finally, compression must be applied to the stomach so that the ulcerated margins of the ulcer are forced together to entrap barium in a curved semilunar configuration, with the convexity directed toward the lumen of the stomach. The lucency that results from the heaped-up walls of the ulcer touching each other is called the Kirkland complex (see figures).






