Case 30
[level-membership-for-internal-medicine-category]
Case 30
A 61-year-old overweight male (6 feet tall, weight 280 pounds) presented with a history of progressively worsening shortness of breath over the last month. At admission, he was found to be in atrial fibrillation. He had a remote history of smoking and recent heavy drinking. He was referred for a pharmacologic stress test. He was taking heparin, aspirin, and digoxin.
He underwent 2-day imaging protocol because of his overweight. Rest imaging was done on the first day, using 30 mCi of technetium-99-sestamibi. He underwent pharmacologic stress using 5-minute adenosine infusion protocol on the second day. His heart rate changed from 101 to 89 beats/min and blood pressure from 178/100 to 189/100. He did not complain of chest pain. His ECG showed atrial fibrillation, left axis deviation, and nonspecific T-wave flattening. There was no further change with adenosine infusion.
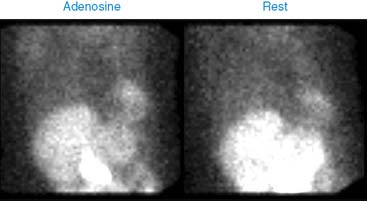
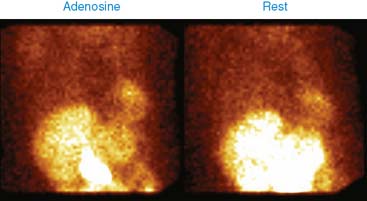
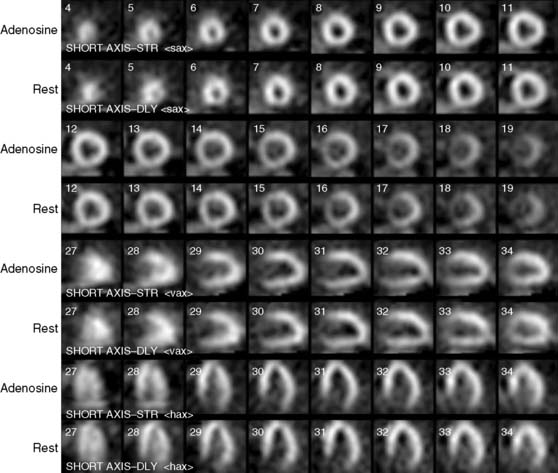
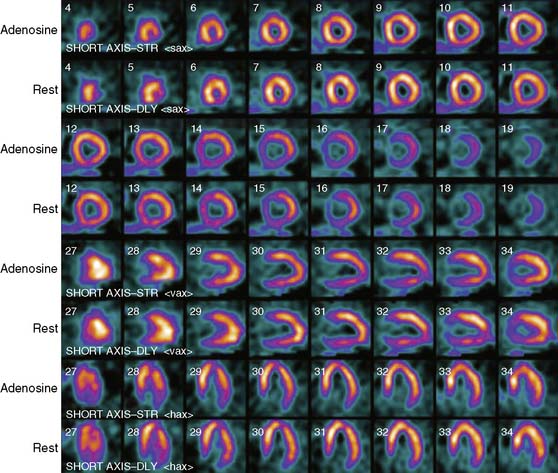
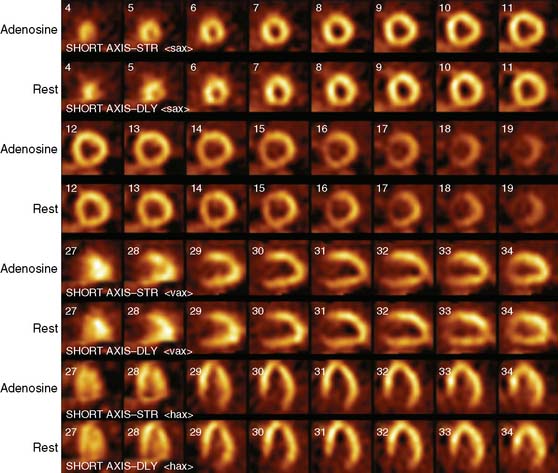
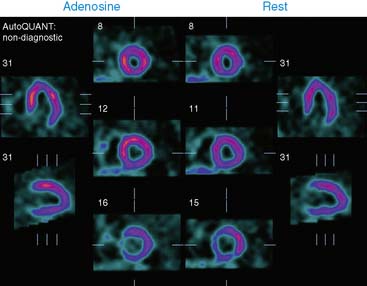
His stress and rest images are shown next. What is your interpretation?
The left ventricle is enlarged, hypertrophied, and hypokinetic. Left ventricular ejection fraction is impaired at 36%, but there is no regional perfusion abnormality.
These findings are consistent with hypertensive heart disease. However, the long history of alcohol abuse and atrial fibrillation with uncontrolled heart rate may have contributed to the LV dysfunction.
He was DC-cardioverted and put on medical therapy with angiotension-converting enzyme (ACE) inhibitors, digoxin, and β-blockers. With good rate control, blood pressure control, and abstinence from alcohol, one should expect improvement in his cardiac function.
[/level-membership-for-internal-medicine-category][not-level-membership-for-internal-medicine-category]
Case 30
A 61-year-old overweight male (6 feet tall, weight 280 pounds) presented with a history of progressively worsening shortness of breath over the last month. At admission, he was found to be in atrial fibrillation. He had a remote history of smoking and recent heavy drinking. He was referred for a pharmacologic stress test. He was taking heparin, aspirin, and digoxin.
He underwent 2-day imaging protocol because of his overweight. Rest imaging was done on the first day, using 30 mCi of technetium-99-sestamibi. He underwent pharmacologic stress using 5-minute adenosine infusion protocol on the second day. His heart rate changed from 101 to 89 beats/min and blood pressure from 178/100 to 189/100. He did not complain of chest pain. His ECG showed atrial fibrillation, left axis deviation, and nonspecific T-wave flattening. There was no further change with adenosine infusion.
Buy Membership for Internal Medicine Category to continue reading.
Learn more here
[/not-level-membership-for-internal-medicine-category]
Clinical Nuclear Cardiology State of the Art and Future Directio