CASE 30
Sam is a 44-year-old, previously healthy man who has been suffering from blurred vision and intermittent numbness in the left leg and right arm for 7 months. Over the past 4 weeks he has been incontinent of urine twice. His male companion is convinced he has a brain tumor or some other sinister disorder. All of his routine blood work is normal, as is his urinalysis, antinuclear antibody (ANA) titers, and complement C3 levels. His last HIV test (6 years ago) was negative, and he has lived with his current partner for more than 5 years. A repeat HIV test is negative.
QUESTIONS FOR GROUP DISCUSSION
RECOMMENDED APPROACH
Implications/Analysis of Clinical History
Infection
Toxoplasmosis (and other chronic CNS infections [e.g., Cryptococcus neoformans]) could present as a multifocal disease. One might expect viral encephalopathies (e.g., herpes simplex virus, also referred to as human herpesvirus 1) to present more acutely than over months. Again, infection is unlikely to be intermittent. Immune complex deposition disease (lupus cerebritis) such as occurs in systemic lupus erythematosus (SLE), is a possibility because it is associated with intermittent inflammation in the CNS (see Case 31).
THERAPY
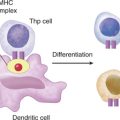
Monoclonal Antibodies
In another approach, CD4+ T cells are targeted with monoclonal antibodies so that complement or phagocytes can destroy them. The specificity of the monoclonal antibodies is the particular Vβ segment present in the T cell receptors that recognize the class II MHC/MS complex (see Case 2). The downside to this approach is that many T cells specific for other peptide-MHC complexes also express that particular Vβ segment and so all of these T cells would also be destroyed.
ETIOLOGY: MULTIPLE SCLEROSIS
MS is a chronic inflammatory disease of the CNS that results in scarring and demyelination (Fig. 30-1). There is evidence that a breakdown of tolerance to a variety of nerve-associated proteins/glycolipids plays a major role in the disease process. CD4+ T cells, secreting type 1 cytokines, have been the focus of investigations and novel therapies for MS. More recently, however, a role for type 2 cytokines (and CD8+ T cells) in the disease process has been proposed. Autoantibodies specific for myelin basic protein are generated in MS, but these are not thought to be the inciting agents of disease. They do, however, contribute to the pathogenesis of disease because their presence can activate phagocytes and complement processes.
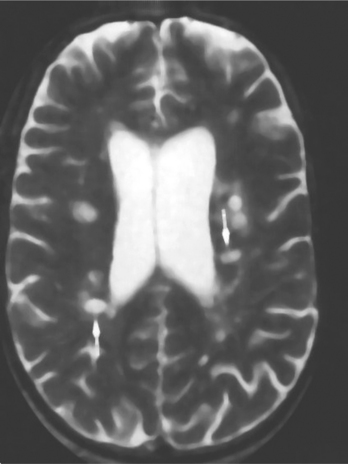
FIGURE 30-1 Multiple periventricular lesions seen in MR image of patient with late-stage multiple sclerosis.
Immunoglobulin Profiles in CNS and Serum
CD4+ T cells recognize unique CNS antigens (e.g., myelin basic protein), and cytokine production from these T cells activates local inflammatory processes. Note that when cells in the immune system are activated by specific antigen, only T and B cells recognizing that particular antigen will proliferate. This results in so-called oligoclonal activation, not polyclonal activation.