Procedure 3 Nail Bed Repair
Indications





Examination/Imaging
Clinical Examination
 Complete sensory examination before anesthesia.
Complete sensory examination before anesthesia.
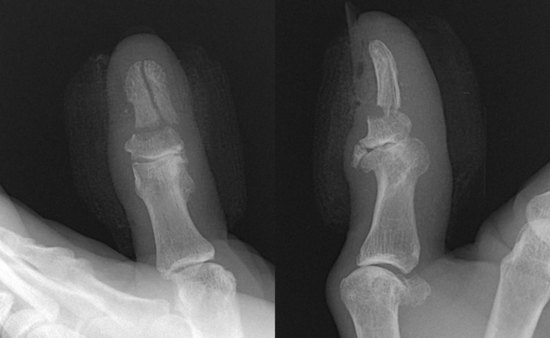
 Note pattern of nail bed laceration (simple/stellate), involvement of germinal matrix, and dorsal roof matrix. (Fig. 3-3 shows a crush injury of the right thumb with a stellate laceration involving the sterile and germinal matrices.)
Note pattern of nail bed laceration (simple/stellate), involvement of germinal matrix, and dorsal roof matrix. (Fig. 3-3 shows a crush injury of the right thumb with a stellate laceration involving the sterile and germinal matrices.)
 Look out for associated subtotal pulp amputation (Fig. 3-4).
Look out for associated subtotal pulp amputation (Fig. 3-4).



Surgical Anatomy
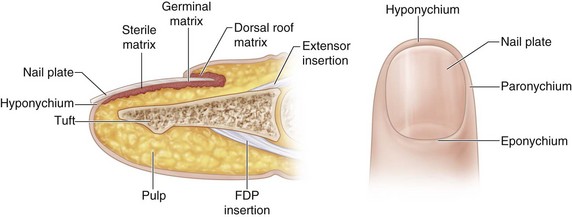
 The nail is a hard structure composed of desiccated, keratinized, squamous cells attached to the nail bed and is the end product of the nail bed’s generative efforts. The nail is loosely attached to the germinal matrix but is densely adherent to the underlying sterile matrix and the eponychium.
The nail is a hard structure composed of desiccated, keratinized, squamous cells attached to the nail bed and is the end product of the nail bed’s generative efforts. The nail is loosely attached to the germinal matrix but is densely adherent to the underlying sterile matrix and the eponychium.
 The nail bed is composed of sterile matrix, germinal matrix, and dorsal roof matrix (Fig. 3-6).
The nail bed is composed of sterile matrix, germinal matrix, and dorsal roof matrix (Fig. 3-6).




Exposures
 A Freer elevator is inserted between the nail plate and the nail bed distally and used to elevate the nail plate off the nail bed from distal to proximal.
A Freer elevator is inserted between the nail plate and the nail bed distally and used to elevate the nail plate off the nail bed from distal to proximal.
 Nail bed lacerations that extend under the nail fold or involve the germinal matrix require elevation of the dorsal roof matrix to expose the laceration and allow a good repair. This is done by making two oblique incisions at the corner of the nail fold and elevating the dorsal roof matrix as a proximally based flap. Two sutures at either corner maintain the flap in position (Fig. 3-7).
Nail bed lacerations that extend under the nail fold or involve the germinal matrix require elevation of the dorsal roof matrix to expose the laceration and allow a good repair. This is done by making two oblique incisions at the corner of the nail fold and elevating the dorsal roof matrix as a proximally based flap. Two sutures at either corner maintain the flap in position (Fig. 3-7).

Pearls
In children, general anesthesia is required to facilitate a meticulous repair.
If the laceration involves only the distal portion of sterile matrix, the nail plate needs to be elevated only 1 to 2 mm beyond the laceration.
Examine the undersurface of the nail for any nail bed remnants. They can be used as a free graft.
When the dorsal roof matrix flap is sutured back, it is important to ensure that the suture passes through the full thickness of the tissue.
Procedure
Step 1

Step 2


Step 2 Pearls
A slight gap is preferable to a tight nail bed repair.
A nail bed graft needs to be considered if there is loss of nail bed or there is a gap larger than 4 to 5 mm in the sterile matrix. A split-thickness sterile matrix graft can be harvested from the great toe without much donor morbidity. A gap in or loss of the germinal matrix is difficult to reconstruct. A sterile matrix graft will not replace the function of the germinal matrix. A germinal matrix graft from the toes will cause loss of nail growth in the toes, and the result at the finger may not be successful. It may be reasonable to consider an amputation of the digit proximal to the germinal matrix. An option in patients desiring germinal matrix reconstruction is transfer of toe pulp, using the nail complex as a free flap.
In severely comminuted stellate nail bed lacerations, it is better to approximate the multiple nail bed flaps with a few strategic sutures instead of attempting an anatomic repair (Fig. 3-9). Good results have been reported with the use of cyanoacrylate glue (Dermabond) in the suturing of such lacerations (Fig. 3-10).


Step 3
 The nail is replaced into the nail fold. A figure-of-eight suture or a simple suture from the nail to hyponychium can be used to hold the nail in place.
The nail is replaced into the nail fold. A figure-of-eight suture or a simple suture from the nail to hyponychium can be used to hold the nail in place.

Step 3 Pearls
A couple of holes should be made in the nail using an 18-gauge needle. This provides space for blood to drain (after the tourniquet is released).
If the nail is unavailable or crushed, a sterile artificial silicone nail or a suture package cut in the shape of the nail can be placed within the nail fold (Fig. 3-11). One should remember to make holes for drainage in these nail inserts also.
The nail or an artificial splint should be placed into the nail fold for all lacerations involving the germinal matrix.

Procedure
Germinal Matrix Avulsion
Step 1
 A transverse laceration of the germinal matrix at the proximal end of the nail bed (at the junction with the dorsal roof matrix) is referred to as an “avulsion of the germinal matrix.” This distally based flap of germinal matrix prolapses out of the nail fold (Fig. 3-12). It is occasionally associated with a displaced fracture of the base of the distal phalanx and prevents closed reduction of the fracture.
A transverse laceration of the germinal matrix at the proximal end of the nail bed (at the junction with the dorsal roof matrix) is referred to as an “avulsion of the germinal matrix.” This distally based flap of germinal matrix prolapses out of the nail fold (Fig. 3-12). It is occasionally associated with a displaced fracture of the base of the distal phalanx and prevents closed reduction of the fracture.


Step 2






Management of Associated Distal Phalangeal Fracture
 Fractures should be fixated before nail bed repair.
Fractures should be fixated before nail bed repair.


 It is better to pin unstable fractures (e.g., transverse fracture between the terminal extensor and flexor insertions). (Figure 3-14 shows intraoperative and late postoperative radiographs of the patient in Figures 3-3 and 3-5.)
It is better to pin unstable fractures (e.g., transverse fracture between the terminal extensor and flexor insertions). (Figure 3-14 shows intraoperative and late postoperative radiographs of the patient in Figures 3-3 and 3-5.)




Postoperative Care and Expected Outcomes
 A nonadherent dressing covered by sterile gauze over a finger dressing is applied.
A nonadherent dressing covered by sterile gauze over a finger dressing is applied.



 Figure 3-15 shows the late result of repair of a simple laceration of the sterile matrix after 3 months.
Figure 3-15 shows the late result of repair of a simple laceration of the sterile matrix after 3 months.
 Figure 3-16 shows the late result of repair of a stellate laceration involving the sterile and germinal matrices of the right index finger after 6 months.
Figure 3-16 shows the late result of repair of a stellate laceration involving the sterile and germinal matrices of the right index finger after 6 months.
 Figure 3-17 shows the late results of repair of the germinal matrix avulsion shown in Figure 3-12 after 6 months.
Figure 3-17 shows the late results of repair of the germinal matrix avulsion shown in Figure 3-12 after 6 months.



Roser SE, Gellman H. Comparison of nail bed repair versus nail trephination for subungual hematomas in children. J Hand Surg [Am]. 1999;24:1166-1170.
Strauss EJ, Weil WM, Jordan C, Paksima N. A prospective, randomized, controlled trial of 2-octylcyanoacrylate versus suture repair for nail bed injuries. J Hand Surg [Am]. 2008;33:250-253.


