CASE 3


History: A patient presents with chest pain.
1. What should be included in the differential diagnosis of a valvular mass? (Choose all that apply.)
A. Angiosarcoma
B. Thrombus
C. Vegetation
D. Myxoma
2. What is the most common valvular tumor?
A. Thrombus
C. Myxoma
D. Angiosarcoma
3. What is the most likely diagnosis?
B. Angioinvasive aspergillosis
4. In regard to this diagnosis, which valve is most commonly affected in intravenous drug users?
A. Aortic valve
B. Mitral valve
ANSWERS
CASE 3
Reference
Feuchtner GM, Stolzmann P, Dichtl W, et al. Multislice computed tomography in infective endocarditis: comparison with transesophageal echocardiography and intraoperative findings. J Am Coll Cardiol. 2009;53(5):436–444.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, p 283.
Comment
Imaging
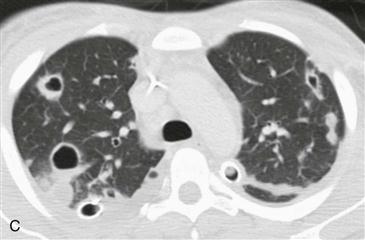
Prospectively gated cardiac CT scan through the level of the tricuspid valve shows an oval-shaped mass (Figs. A and B). CT scan at a higher level with lung windows (Fig. C) shows multiple peripherally located cavitary lung nodules. This patient was an intravenous drug user who presented with high fever and sepsis. Findings are consistent with septic pulmonary embolism from a tricuspid valve vegetation.
Differential Diagnosis
The differential diagnosis for a valvular mass is limited. In the setting of intravenous drug use, the most common valvular mass is a vegetation. Gated CT is both sensitive and specific for detecting a valvular vegetation in patients with suspected endocarditis. CT may be better suited than transesophageal or transthoracic echocardiography to help with surgical planning because it better delineates the anatomic structures involved by a potential perivalvular abscess or pseudoaneurysm. In the absence of infectious symptoms, a valvular mass is most likely tumor or thrombus. The most common valvular tumor is papillary fibroelastoma. This tumor may be seen only on echocardiography because it is usually small (<1 cm) and very mobile. A valvular tumor is best differentiated from valvular thrombus because a tumor demonstrates contrast enhancement on either CT or MRI.






