[level-membership-for-surgery-category]
Procedure 29 Release of a Spastic Elbow Flexion Contracture
 See Video 22: Biceps and Brachialis Lengthening
See Video 22: Biceps and Brachialis Lengthening

Examination/Imaging
Clinical Examination
 The three major causes of an elbow flexion contracture resulting from spasticity are cerebral palsy, stroke, and traumatic brain injury. There are some differences in the approach to treatment among these three causes.
The three major causes of an elbow flexion contracture resulting from spasticity are cerebral palsy, stroke, and traumatic brain injury. There are some differences in the approach to treatment among these three causes.




Surgical Anatomy
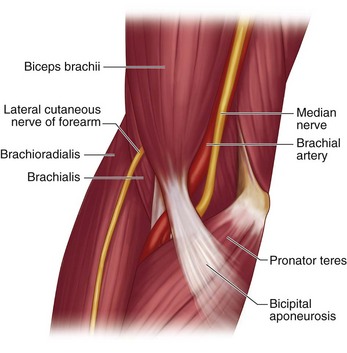
 The cubital fossa, bounded medially by the pronator teres and laterally by the brachioradialis, contains the lateral cutaneous nerve of the forearm, the tendon of the biceps brachii, the brachial artery, and median nerve. The brachial artery and median nerve are located medial to the biceps brachii, and the lateral cutaneous nerve of the forearm is lateral to the biceps brachii. The lacertus fibrosus, also known as the bicipital aponeurosis, continues distally as deep fascia of the forearm (Fig. 29-1).
The cubital fossa, bounded medially by the pronator teres and laterally by the brachioradialis, contains the lateral cutaneous nerve of the forearm, the tendon of the biceps brachii, the brachial artery, and median nerve. The brachial artery and median nerve are located medial to the biceps brachii, and the lateral cutaneous nerve of the forearm is lateral to the biceps brachii. The lacertus fibrosus, also known as the bicipital aponeurosis, continues distally as deep fascia of the forearm (Fig. 29-1).
Positioning


Exposures
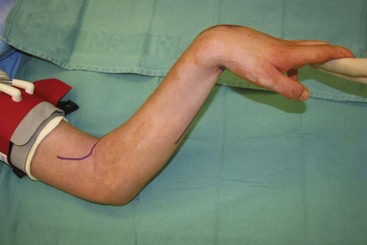
 A 15-cm long “lazy S”–shaped incision is made over the antecubital fossa. The incision begins on the lateral aspect of the arm over the origin of the brachioradialis muscle and gently curves over the antecubital crease distally toward the anteromedial aspect of the forearm (see Fig. 29-2).
A 15-cm long “lazy S”–shaped incision is made over the antecubital fossa. The incision begins on the lateral aspect of the arm over the origin of the brachioradialis muscle and gently curves over the antecubital crease distally toward the anteromedial aspect of the forearm (see Fig. 29-2).
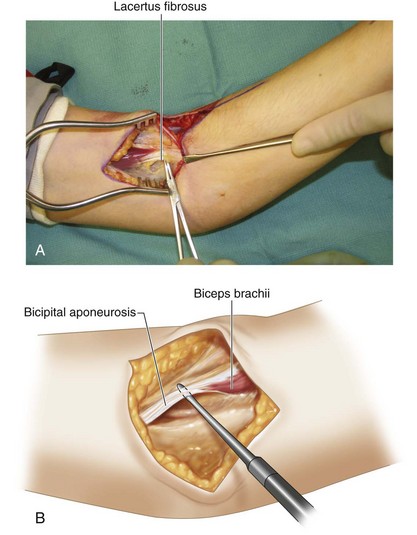
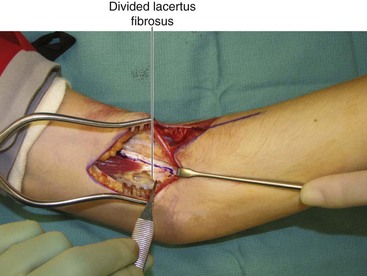
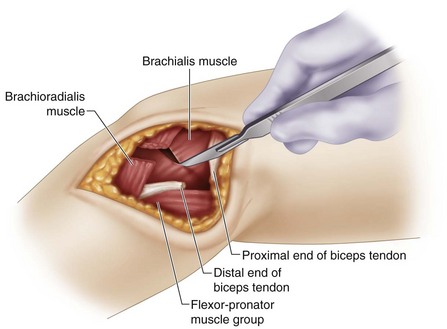
 The subcutaneous dissection is continued from medial to lateral, to expose the cubital fossa. The lacertus fibrosus and the biceps brachii tendon are identified (Fig. 29-3A and B). The median nerve and brachial artery are identified medial to the biceps tendon, and the lateral antebrachial cutaneous nerve is identified lateral to the biceps tendon emerging from the interval between the biceps and brachialis.
The subcutaneous dissection is continued from medial to lateral, to expose the cubital fossa. The lacertus fibrosus and the biceps brachii tendon are identified (Fig. 29-3A and B). The median nerve and brachial artery are identified medial to the biceps tendon, and the lateral antebrachial cutaneous nerve is identified lateral to the biceps tendon emerging from the interval between the biceps and brachialis.
Procedure
Step 1

Step 2
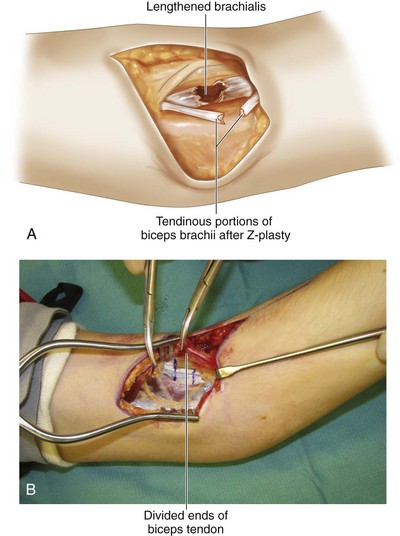
 The contracted biceps brachii is exposed and dissected distal to its insertion. The decision regarding the degree of biceps lengthening should be made at this time. A fractional lengthening is performed for mild contractures, and a Z-lengthening is performed for more severe contractures.
The contracted biceps brachii is exposed and dissected distal to its insertion. The decision regarding the degree of biceps lengthening should be made at this time. A fractional lengthening is performed for mild contractures, and a Z-lengthening is performed for more severe contractures.

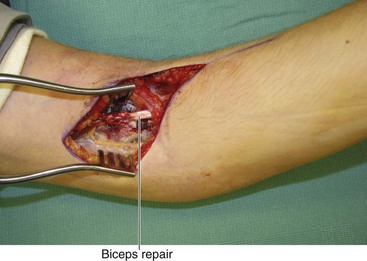
 A Z-lengthening (step-cut) is performed over as much length of the tendon as possible because this gives more tendon substance to do a strong repair (see Fig. 29-4).
A Z-lengthening (step-cut) is performed over as much length of the tendon as possible because this gives more tendon substance to do a strong repair (see Fig. 29-4).
Step 3
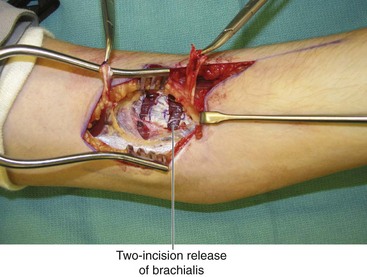
 The release of the biceps brings the brachialis into view. Depending on the degree of contracture and the volitional control of the patient, a partial or complete release of the brachialis can be done.
The release of the biceps brings the brachialis into view. Depending on the degree of contracture and the volitional control of the patient, a partial or complete release of the brachialis can be done.
 A partial release can be done using one or two incisions (Fig. 29-5A). A double incision gives more release. A transverse incision is made over the aponeurotic portion on the anterior aspect of the muscle, leaving the muscle intact. If two incisions are used, they are spaced about 1 to 2 cm apart (Fig. 29-5B).
A partial release can be done using one or two incisions (Fig. 29-5A). A double incision gives more release. A transverse incision is made over the aponeurotic portion on the anterior aspect of the muscle, leaving the muscle intact. If two incisions are used, they are spaced about 1 to 2 cm apart (Fig. 29-5B).

Step 4
 At this point, assessment of the brachioradialis is done. A partial or complete release of the brachioradialis can be performed, depending on the degree of spasticity and the volitional control of the patient. Dissection is carried out between the brachialis and the brachioradialis.
At this point, assessment of the brachioradialis is done. A partial or complete release of the brachioradialis can be performed, depending on the degree of spasticity and the volitional control of the patient. Dissection is carried out between the brachialis and the brachioradialis.
Step 4 Pearls
If the brachioradialis has volitional control and the elbow contracture is not very severe, a partial release can be done through a separate 3-cm longitudinal incision made on the dorsoradial aspect of the mid-forearm. The tendinous portion of the brachioradialis is on its deeper surface; the muscle needs to be reflected to visualize this portion. A transverse incision is used to divide only the tendon, keeping the muscle in continuity.




Postoperative Care and Expected Outcomes
 A long-arm plaster of Paris splint that keeps the elbow at 30 degrees of flexion is applied.
A long-arm plaster of Paris splint that keeps the elbow at 30 degrees of flexion is applied.

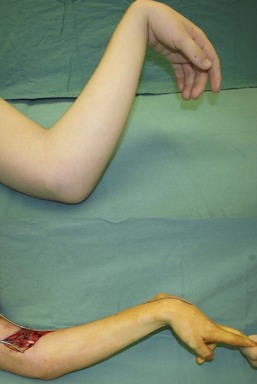
 Patients who undergo fractional lengthening of the biceps can expect a 10- to 30-degree improvement in the flexion contracture without appreciable loss of flexion power. Patients who undergo Z-lengthening can expect up to a 45- to 60-degree improvement in flexion contracture, but they do lose elbow flexion power. It is important to avoid full extension of the elbow in patients with volitional control because difficulty with elbow flexion after a full release may become a greater problem for the patient (Fig. 29-9).
Patients who undergo fractional lengthening of the biceps can expect a 10- to 30-degree improvement in the flexion contracture without appreciable loss of flexion power. Patients who undergo Z-lengthening can expect up to a 45- to 60-degree improvement in flexion contracture, but they do lose elbow flexion power. It is important to avoid full extension of the elbow in patients with volitional control because difficulty with elbow flexion after a full release may become a greater problem for the patient (Fig. 29-9).
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
Procedure 29 Release of a Spastic Elbow Flexion Contracture
See Video 22: Biceps and Brachialis Lengthening
Examination/Imaging
Clinical Examination
The three major causes of an elbow flexion contracture resulting from spasticity are cerebral palsy, stroke, and traumatic brain injury. There are some differences in the approach to treatment among these three causes.
