CASE 29

History: A 44-year-old man presents with dysphagia.
1. Which of the following should be included in the likely differential diagnosis of the imaging findings? (Choose all that apply.)
B. Esophageal squamous cell carcinoma
C. Primary esophageal lymphoma
E. Gastric squamous cell carcinoma
2. What is the most common type of malignancy seen at the gastroesophageal junction?
3. There are non-neoplastic processes that could give this appearance of a mass at the gastro-esophageal junction. Which of the following would not be expected to give this appearance?
4. What inflammatory process is a predisposing factor associated with this lesion?
D. Helicobacter pylori gastritis
ANSWERS
CASE 29
Adenocarcinoma of the Gastroesophageal Junction
1. A, B, and D
2. A
3. A
4. B
References
Iyer R, Dubrow R. Imaging upper gastrointestinal malignancy. Semin Roentgenol. 2006;41:105–112.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, pp 23-26.
Comment
A tumor at the gastroesophageal (GE) junction may have arisen from the stomach or from the esophagus. The gastric tumors are nearly always adenocarcinomas. Of the tumors arising from the esophagus, squamous cell carcinoma was by far the most common (80% to 90%). However, the incidence of adenocarcinoma of the esophagus has increased almost 500% in the Western world since 1980.
This change is due directly to the increased incidence of Barrett’s metaplasia, now seen in the distal esophagus. Patients with Barrett’s metaplasia have a 40% or greater risk of malignancy, and almost all adenocarcinomas of the distal esophagus and gastroesophageal junction are a result of pre-existing Barrett’s metaplasia. These patients are usually younger than those with the typical squamous cell lesion of the esophagus. They often have a long history of heartburn symptoms and present with dysphagia to solid foods. The correlating factors of smoking and alcohol seen with squamous cell carcinoma might not apply to this lesion. Although almost all adenocarcinomas arise from underlying dysplastic disease (Barrett’s), a tiny percentage might arise from the sparse adenomatous glands of the esophagus directly. In general, the more distal the lesion, the more lightly the predisposing factor is Barrett’s metaplasia.
The 5-year survival rate in general for this lesion is 10% to 12%, but this, too, is to a great extent related to the spread of the disease. It can be very local, it can spread via the adjacent lymph node chain (upper celiac in the gastrohepatic ligament), or it can occur with distal metastatic disease to the lung and elsewhere.
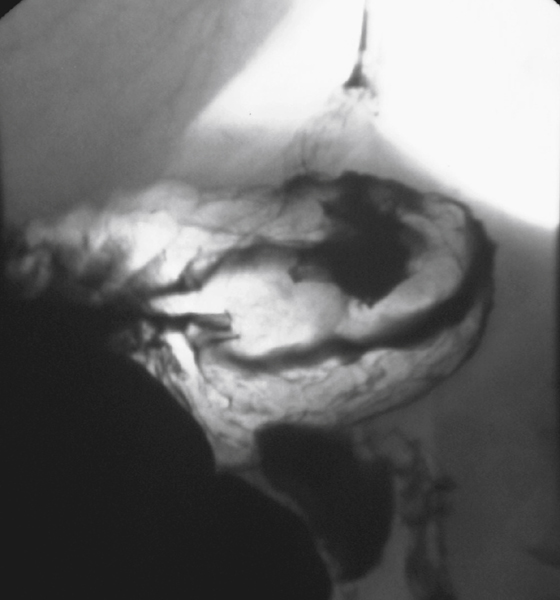
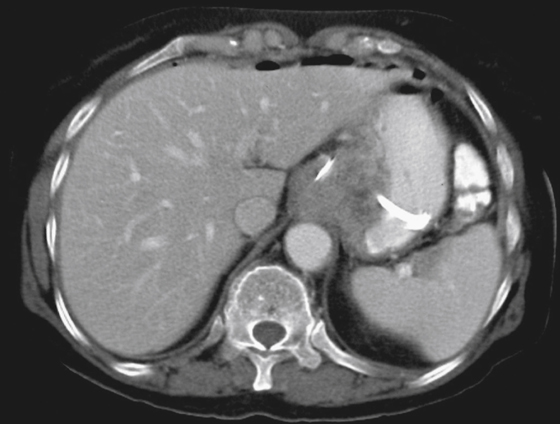
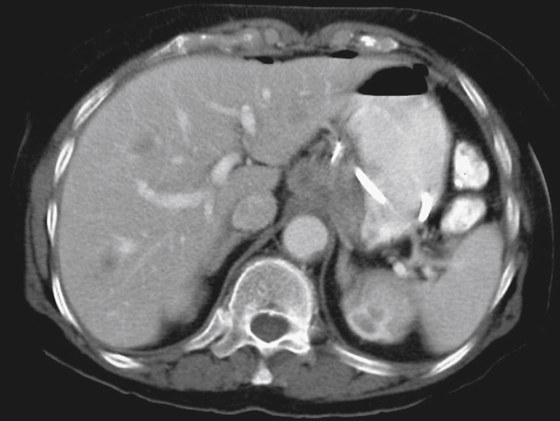
Radiologic findings include mass, narrowing, and irregularity at the GE junction (see figures). This may be associated with some chronic inflammatory changes on barium studies. CT images reveal a thickened esophageal wall (greater than 5 mm) as well as the possibility of nodes in the mediastinum and paragastric areas (see figures).






