CASE 29

1. What should be included in the differential diagnosis? (Choose all that apply.)
A. Fibrosis
B. Pneumonia
D. Acute respiratory distress syndrome
2. What is the predominant distribution of the lung opacity?
A. Basilar
B. Upper lobe
C. Peripheral
D. Perihilar
3. What is the most likely diagnosis?
A. Fibrosis
B. Pneumonia
D. Acute respiratory distress syndrome
4. What is the most likely etiology?
A. Cardiogenic
B. Neurogenic
ANSWERS
Reference
Eisenhuber E, Schaefer-Prokop CM, Prosch H, et al. Bedside chest radiography. Respir Care. 2012;57(3):427–443.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, p 18.
Comment
Pathophysiology and Etiology
Pulmonary edema can be related to both blood flow and blood pressure or to blood pressure alone. Elevation of pulmonary venous pressure can be secondary to left ventricular failure, mitral stenosis, and other causes of vascular obstruction distal to the pulmonary arterial bed.
Imaging Findings
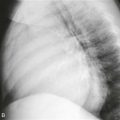
When pressure increases, pulmonary blood flow is redistributed to the upper lobes, which manifests as enlargement of the upper lobe vessels (“cephalization”) on chest radiographs. When pulmonary venous pressure increases further, pulmonary interstitial edema ensues. Kerley B lines—thin, horizontal, interlobular septal lines—are seen at the lung bases on chest radiographs. With further elevation of pulmonary venous pressure, alveolar edema develops, and chest radiographs may demonstrate opacities that involve the central portions of the lungs, sometimes producing a “bat wing” appearance (Figure). If the pulmonary edema is related to congestive heart failure, the cardiac silhouette is enlarged, and pleural effusions are often seen on chest radiographs.