CASE 28
History: A 30-year-old woman with bulimia presented after a bulimic binge of 10 liters of water with collapse and abdominal distention. Emergency laparotomy was performed where the stomach appeared viable and a gastrostomy tube was placed. She deteriorated over the next 2 weeks.
1. What conditions can be associated with this finding? (Choose all that apply.)
E. Endoscopy (especially with intervention)
2. Some infectious processes are recognized to produce this abnormality. Which of these agents is not known to cause this abnormality?
3. Ingestion of what type of substance can cause this problem?
4. What is the most common location for intramural gas to occur in the gastrointestinal tract?
ANSWERS
CASE 28
Emphysematous Gastritis
1. A, B, C, and E
2. D
3. C
4. C
References
Lee S. Gastric emphysema. Am J Gastroenterol. 1984;79(11):899–904.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 88.
Comment
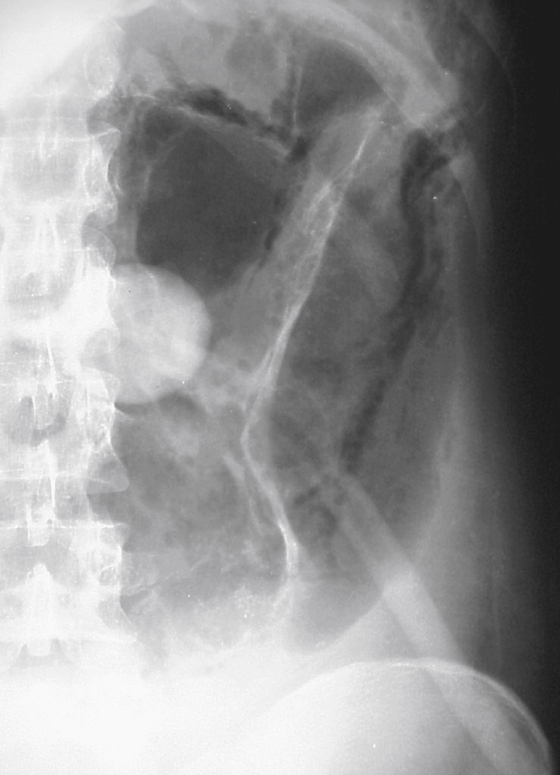
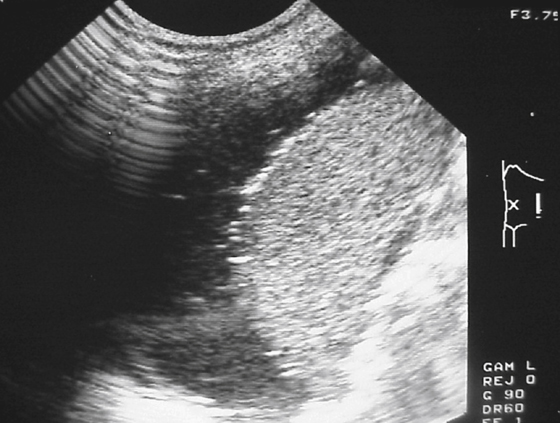
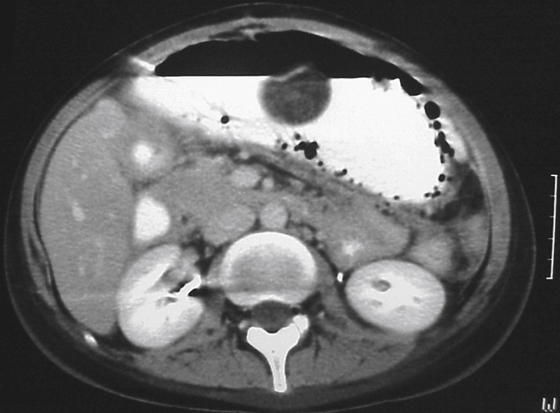
The finding of air in the wall of the stomach is quite often an ominous sign (see figures). Although air in the stomach wall can be a sequela of recent endoscopy or gastric surgery, it is a rare complication. Despite the thousands of endoscopic procedures performed, a radiologist rarely encounters air in the gastric wall as a result of them.
Most commonly the occurrence of air in the wall represents a severe infection of the stomach, a type of phlegmonous gastritis. Although many organisms have been isolated in these infections, the most common are hemolytic streptococci, Clostridium welchii, and coliform bacteria. Infection may be slightly more common in severe diabetes, relating to the overall systemic disease process as well as local diabetes-induced vasculitides. Infection has been identified in otherwise healthy patients, as well as in those with a variety of chronic, debilitating conditions (e.g., transplant recipients, postoperative patients, those with AIDS). The process by which the infection develops is uncertain, but it is believed that ulcers or other breaks in the mucosa allow bacteria access to the submucosal tissue, with resultant spread of infection. Discovery of phlegmonous gastritis probably indicates impending necrosis of the gastric wall. Prompt therapy, including gastrectomy and antibiotics, is necessary because the mortality rate is quite high.
Emphysematous gastritis also can be encountered in patients with gastric outlet obstruction, in whom elevated intraluminal pressures can force air into the gastric wall. Rarely, the condition is seen in patients with pulmonary disease who also develop pneumatosis in other parts of the gastrointestinal tract.
Patients who ingest corrosive agents in an attempt to commit suicide also can develop this complication, which heralds necrosis of the gastric wall. As is true of other radiologic findings, the clinical history is the most important factor in establishing the correct diagnosis.






