Case 28
Case 28
The patient is an 81-year-old male with type 2 diabetes, hypertension, hyperlipidemia, and myocardial infarction 30 years earlier. He did not consent to cardiac catheterization and never underwent catheterization or revascularization. He is currently doing well and is physically active with normal exercise tolerance. He was referred for a routine stress/rest 99mTc-sestamibi perfusion imaging study.
Medications: pravastatin, nadolol, lisinopril, nifedipine, aspirin, and metformin.
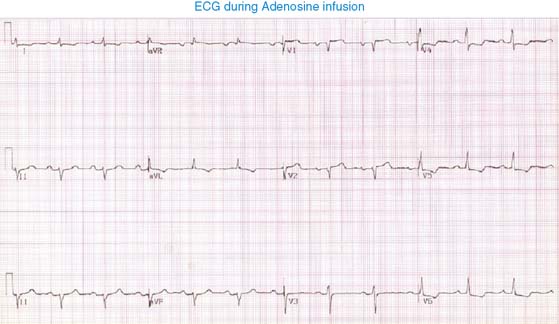
Pharmacologic stress perfusion imaging using 5-minute adenosine infusion was performed, and the following changes were noted: heart rate rose from 60 to 70 beats/min and blood pressure dropped from 130/90 to 125/61. The patient reported no chest pain.
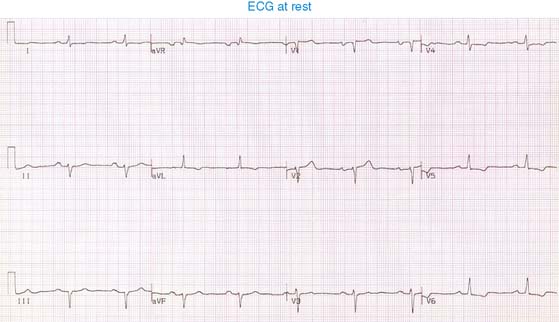
Baseline ECG shows normal sinus rhythm, first degree AV block left atrial enlargement, and possibly old inferior wall infarction and generalized ST-T changes. With adenosine infusion, there is 1.5-mm ST-segment depression in leads V4-5, which recovers within 3 minutes of termination of the infusion. Given the baseline ECG changes, this is a nonspecific ST-segment change.
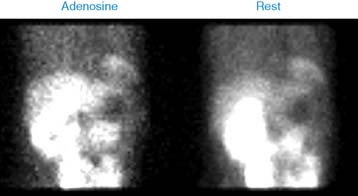
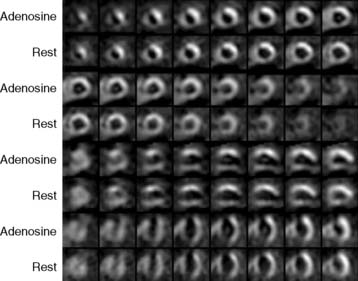
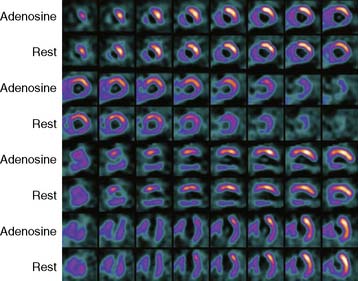
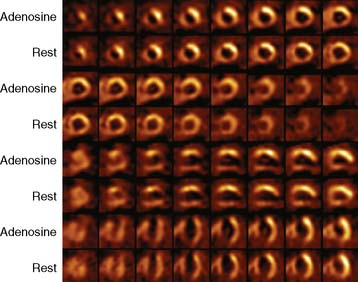
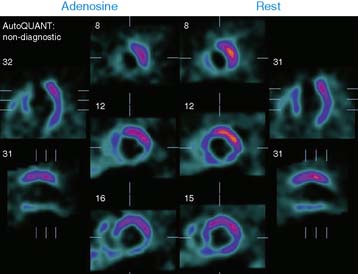
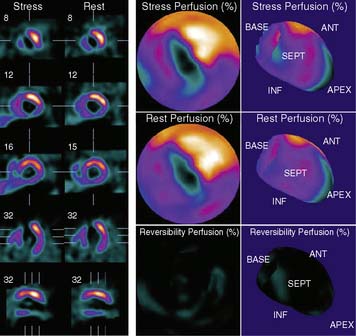
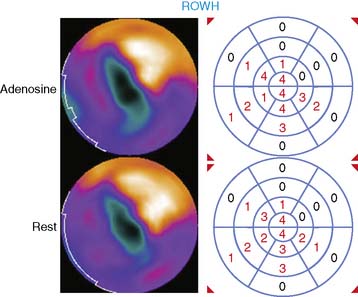
The left ventricle is enlarged, and there is a large, dense scar involving the septum, apex, inferior wall, and contiguous lateral wall, with no reversibility. The septum and inferior wall are severely hypokinetic, and LVEF is depressed at 34%.
Despite a large scar, the patient is doing quite well. He is on optimal medical management.
Clinical Nuclear Cardiology State of the Art and Future Directio