Case 26
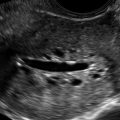
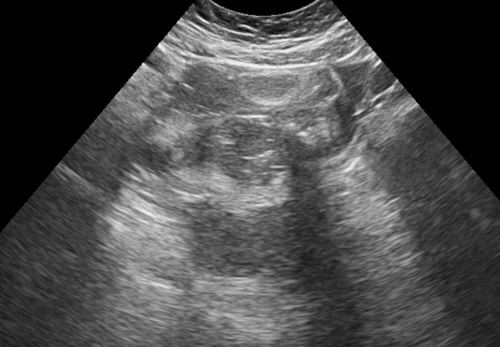
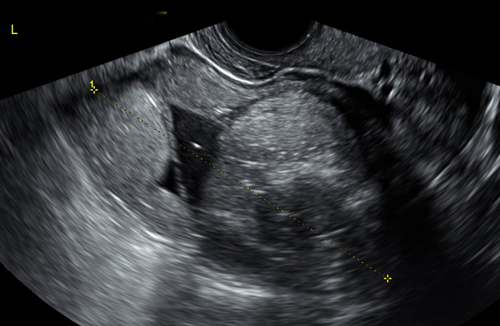
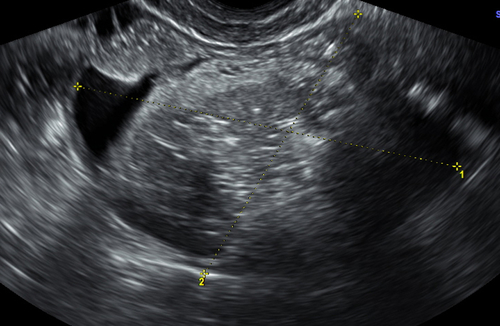
This 25-year-old woman presented with an enlarged uterus on physical examination. The first image (top left) is a transabdominal view of the pelvis. The other images were taken transvaginally.

Case 1 Answer: This mass was mistaken for an ovarian fibroma but was proven to be a mature teratoma at surgery.
Case 2 Answer: Endometriosis involving the back of the cervix and anterior wall of the recto-sigmoid. There was severe focal tenderness at the site of the abnormality during the scan.
Case 3 Answer: Mucocele of the appendix. Note the onion skin–like texture of the internal contents of the lesion. A separate right ovary that appeared normal was documented.
Case 4 Answer: Bilateral cystadenomas of low malignant potential (borderline tumor). Note that these masses with abundant color flow are worrisome for malignancy.
Case 5 Answer: The initial scan suggested a polyp due to the thick, heterogeneous, and cystic central endometrial echo. When saline was infused into the uterine cavity, the mucosal surface appeared thin, compatible with atrophy. The cystic areas are sub-endometrial, which is typical of the Tamoxifen effect and represents glandular cystic atrophy.
Case 6 Answer: Urethral diverticulum. The scans were all done from the perineum, looking down the length of the urethra and vagina. The location of the diverticulum is best seen on the 3-D reconstructed view of the perineum and forms a semilunar shape around the anterior aspect of the urethra.
Case 7 Answer: Retained products of conception. Note the extreme vascularity, which is very common when the abortion is incomplete. This vascularity will resolve completely after a D&C.
Case 8 Answer: Endometriosis of the posterior bladder wall and anterior aspect of the uterus. Note the mass-like thickening of the floor of the bladder (calipers) with involvement of the wall of the uterus underneath.
Case 9 Answer: Degenerating fibroid. The appearance of this mass was nonspecific and more suggestive of an ovarian lesion. The correct diagnosis was not suspected preoperatively because this appearance is atypical for a fibroid, even with degeneration.
Case 10 Answer: This is a thickened endometrium, worrisome for malignancy. The final pathologic diagnosis was grade 2 endometrial adenocarcinoma. Note the vascular mass involving the endometrium and invading the anterior myometrium as well as the echogenic fluid within the cavity (blood).
Case 11 Answer: Dysgerminoma measuring 20 cm × 12 cm.
Case 12 Answer: Acute appendicitis. Note that the appendix has a cystic area in its tip and is surrounded by very echogenic tissue, which represents inflammation of the surrounding fat. A separate, normal right ovary was clearly identified.
Case 13 Answer: Large cervical carcinoma. The first image (top left) shows the measurement of the endometrium, and the second image (top right) shows the calipers on the cervical mass. Note the extreme vascularity.
Case 14 Answer: Intramural choriocarcinoma. The tumor was confined to the myometrium and not contiguous with the endometrial cavity. The patient was treated with chemotherapy to no avail and eventually underwent a hysterectomy for definitive therapy. The tissue typing of the tumor was different from the original choriocarcinoma, consistent with a second, primary choriocarcinoma as opposed to a recurrence.
Case 15 Answer: Decidualized endometrioma.
Case 16 Answer: Left cornual pregnancy. Note how the 3-D coronal image best demonstrates the location of the pregnancy.
Case 17 Answer: Tarlov’s cysts along the anterior aspect of the sacrum bilaterally. The normal ovaries were identified separately.
Case 18 Answer: Right dermoid cyst.
Case 19 Answer: Nodular, deep-penetrating endometriosis of the anterior wall of the recto-sigmoid, behind the distal end of the cervix. The cul-de-sac was frozen with endometriotic implants.
Case 20 Answer: Serous cystadenoma of low malignant potential (borderline tumor). Note the few internal mural nodules containing neovascularity seen by color flow Doppler.
Case 21 Answer: Bladder diverticulum. Note the connection to the bladder on the bottom image.
Case 22 Answer: Hemorrhagic cyst with retracting clot over the course of 3 weeks. Note that the initial scan suggested a solid mass, but this was an avascular clot and was seen to retract 3 weeks later. In addition, the blood flow was only seen peripherally.
Case 23 Answer: Fibrothecoma of the ovary. Note the solid texture with limited blood flow as well as the multiple vertical shadowing stripes (Venetian blind appearance) characteristic of fibromas.
Case 24 Answer: (Hint: The patient had a positive pregnancy test). Complete molar pregnancy. Note that without the complete history, the sonographic appearance could be confused with an endometrial polyp or other endometrial process.
Case 25 Answer: Pelvic inflammatory disease with pyosalpinx. This was thought to be a complication resulting from a micro-perforation during a colonoscopy and was treated with broad-spectrum antibiotics.
Case 26 Answer: Large dermoid located above the uterine fundus. The location of the dermoid likely simulated an enlarged uterus clinically; however, the uterus was normal.