Procedure 25 Flexor Pronator Slide
Indications



Examination/Imaging


Surgical Anatomy




Exposures
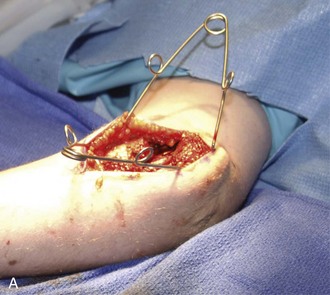
 An anteromedial, longitudinal incision at the elbow situated over the medial epicondyle (Fig. 25-1) is made.
An anteromedial, longitudinal incision at the elbow situated over the medial epicondyle (Fig. 25-1) is made.


Pearls
It may be difficult to establish a plane between the flexor-pronator fascia and the subcutaneous tissue. There are multiple perforating vessels to the dermal layer that will require coagulation.
The dissection needs to extend to the median nerve as it enters between the deep and superficial heads of the pronator teres. This is similar to the exposure for a submuscular ulnar nerve transposition.
Procedure
Step 1
 The ulnar nerve is identified proximal to the medial epicondyle, and a decompression is performed through to the deep flexor carpi ulnaris muscle fibers.
The ulnar nerve is identified proximal to the medial epicondyle, and a decompression is performed through to the deep flexor carpi ulnaris muscle fibers.


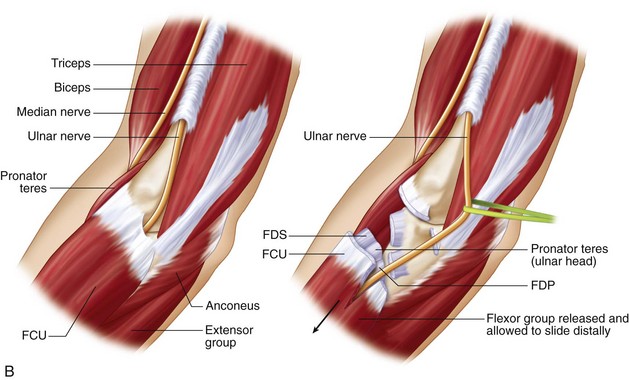
 The entire flexor-pronator mass is then dissected from the medial epicondyle origin. It is elevated from the anterior elbow capsule and proximal portion of the intraosseous membrane (Fig. 25-2).
The entire flexor-pronator mass is then dissected from the medial epicondyle origin. It is elevated from the anterior elbow capsule and proximal portion of the intraosseous membrane (Fig. 25-2).

 Dissection extends to the deep portion of the muscle origin.
Dissection extends to the deep portion of the muscle origin.

Step 1 Pearls
Identify the ulnar nerve proximally and release the cubital tunnel in a distal direction.
The deep dissection will permit identification of the medial collateral ligament. In cases of an elbow contracture, it may be difficult to separate the structure.
The flexor-pronator muscle group needs to be sufficiently mobilized from the elbow capsule and ligament such that the ulnar nerve can be transposed.




Postoperative Care and Expected Outcomes
 The forearm and hand are immobilized with long-arm dorsal and volar splints that hold the fingers and wrist in near full extension, with concomitant elbow extension and forearm supination.
The forearm and hand are immobilized with long-arm dorsal and volar splints that hold the fingers and wrist in near full extension, with concomitant elbow extension and forearm supination.
 After the swelling subsides, the splint can be changed into a cast.
After the swelling subsides, the splint can be changed into a cast.

 There is gradual transition of the splint to a night-time splint over the next several months.
There is gradual transition of the splint to a night-time splint over the next several months.



