CHAPTER 25 Central Venous Catheterization and Pressure Monitoring
1 Define central venous catheterization
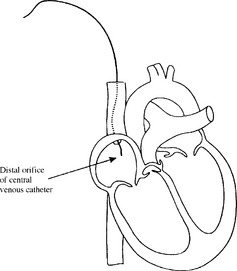
Central venous catheterization involves inserting a catheter into the venous circulation and advancing it so its distal orifice is positioned immediately adjacent to or within the right atrium of the heart (Figure 25-1).












6 Describe the internal jugular vein approach



11 In attempting a central venous puncture, dark blood returns. Does this satisfy you that you are indeed within a vein?
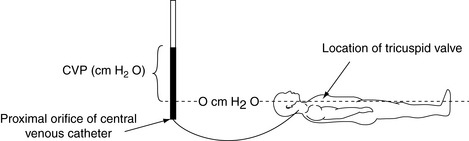
13 At what point on the body should central venous pressure be measured?
An external landmark for the tricuspid is a point 2 inches behind the sternum, roughly the anterior axillary line, at the fourth intercostal space. Ongoing adjustment is necessary to ensure that the transducer or manometer is consistently at this level whenever the patient’s position or bed height is changed (Figure 25-2).
15 How can you judge the correct positioning of the distal orifice of the catheter?



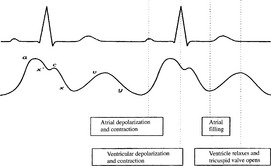
16 Describe the normal central venous pressure waveform and relate its pattern to the cardiac cycle
The normal CVP waveform shows a pattern of three upstrokes and two descents that correspond to certain events in the cardiac cycle (Figure 25-3).












19 How does central venous pressure relate to right ventricular preload?
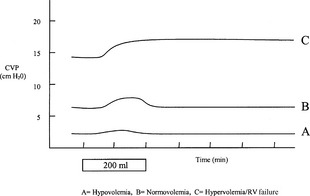
Despite the previous findings, it is widely held that CVP measurement is useful to the clinician as a guide to intravenous fluid replacement, especially at the upper and lower range of CVP. Thus a low (0 to 2 mm Hg) or decreasing CVP may indicate a need for fluid administration, whereas an increasing or elevated CVP (above 12 mm Hg) may indicate overresuscitation or a patient with impaired cardiac performance. The response of CVP to a fluid bolus has also been shown to be useful in assessing fluid status. In Figure 25-4 it can be seen that a 200-ml fluid bolus in the hypovolemic patient will result in a small but transient increase in CVP, whereas the same bolus in the normovolemic patient will result in a larger but still transient increase. However, in the hypervolemic patient with right ventricular failure, the same bolus results in a sustained increase in CVP. The CVP is best used to monitor a trend; an isolated determination is of limited value.
KEY POINTS: Central Venous Catheterization and Pressure Monitoring 
22 Are there noninvasive alternatives to central venous pressure that better indicate volume status?
23 How can an abnormal central venous pressure waveform be used to diagnose abnormal cardiac events?
25 Describe complications associated with placement of the central venous catheter







1. Deflandre E., Bonhomme V., Hans P. Delta down compared with delta pulse pressure as an indicator of volaemia during intracranial surgery. Br J Anaesth. 2008;100:245-250.
2. Domino K.B., Bowdle T.A., Posner K.L., et al. Injuries and liability related to central vascular catheters: a closed claims analysis. Anesthesiology. 2004;100:1411-1418.
3. Gelman S. Venous function and central venous pressure. Anesthesiology. 2008;108:735-748.
4. Taylor R.W., Palagiri A.V. Central venous catheterization. Crit Care Med. 2007;35:1390-1396.
