Published on 02/03/2015 by admin
Filed under Internal Medicine
Last modified 22/04/2025
This article have been viewed 1281 times
Case 25
A 42-year-old male with hypertension and end-stage renal disease complains of chest pain. Medications: hydrochlorothiazide, amlodipine, metoprolol, clonidine, and hydralazine.
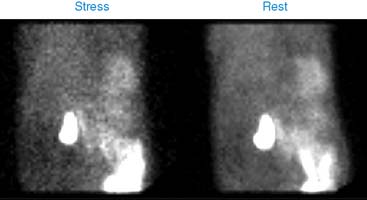
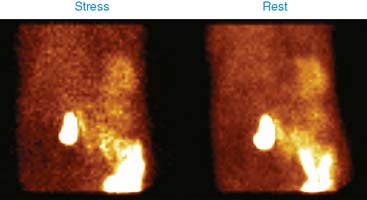
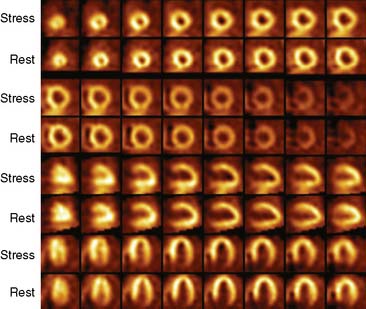
A 5-minute adenosine infusion stress test was performed. 99mTc-sestamibi was used for stress and rest images are shown next. His heart rate changed from 71 to 87 beats/min and blood pressure from 183/87 to 206/85 mm Hg. There was no chest pain. ECG showed normal sinus rhythm, generalized nonspecific ST-T changes, and no further change with adenosine infusion.
(Fig. 1a)
(Video 1a)
(Video 1b)
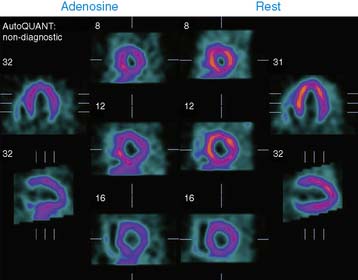
(Fig. 2a)
(Fig. 2b)
(Fig. 2c)
(Video 2)
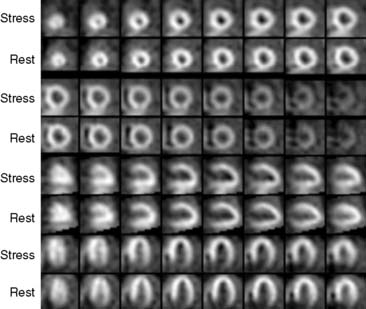
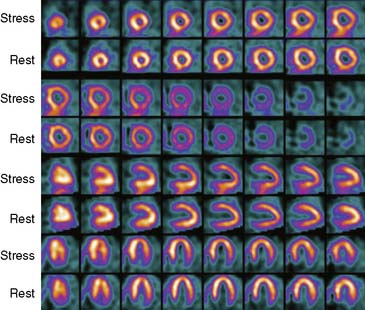
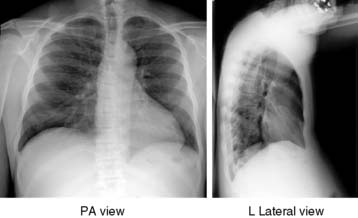
Left ventricle is enlarged and hypertrophied, but there is no regional perfusion abnormality. Left ventricular ejection fraction is marginally impaired at 47%. Myocardial perfusion imaging (MPI) findings are consistent with hypertensive heart disease, but there is no evidence of coronary artery disease. There are large photopenic masses in both flanks of the abdomen. These are consistent with polycystic kidney disease. The diaphragm is pushed superiorly, and intestinal loops are pushed toward the midline. The patient was cleared for renal transplant based upon no perfusion abnormalities on MPI.
(Fig. 3)
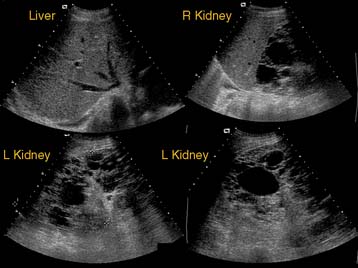
(Fig. 4)
Ultrasound of the abdomen showed that the liver and pancreas were unremarkable, but the kidneys were enlarged and had numerous cysts of various sizes, consistent with polycystic kidney disease. Six months later, the patient required bilateral nephrectomy because of persistent abdominal discomfort and pain from massively enlarged native kidneys. Histopathology of kidneys was consistent with polycystic kidney disease.
FURTHER READING
Ghanbarinia A., Chandra S., Chhabra K., Jain D. Renal abnormalities as incidental findings on myocardial single-photon emission computed tomography perfusion imaging. Nucl Med Commun. 2008;29(7):588-592.
Clinical Nuclear Cardiology State of the Art and Future Directio
WhatsApp us