Procedure 24 Superficialis-to-Profundus Tendon Transfer
Indications




Examination/Imaging



Surgical Anatomy
 Pertinent surgical structures include all volar forearm muscles (palmaris longus, flexor carpi radialis [FCR], flexor carpi ulnaris [FCU], flexor digitorum superficialis [FDS], flexor digitorum profundus [FDP], pronator teres, pronator quadratus), median nerve, ulnar nerve and artery, and radial artery.
Pertinent surgical structures include all volar forearm muscles (palmaris longus, flexor carpi radialis [FCR], flexor carpi ulnaris [FCU], flexor digitorum superficialis [FDS], flexor digitorum profundus [FDP], pronator teres, pronator quadratus), median nerve, ulnar nerve and artery, and radial artery.


Exposures
 A longitudinal volar forearm approach from the mid-forearm to the proximal wrist crease is used.
A longitudinal volar forearm approach from the mid-forearm to the proximal wrist crease is used.
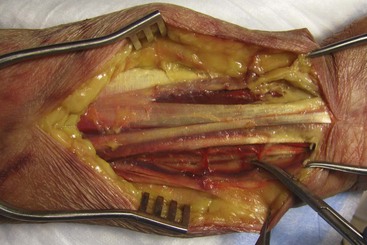
 The FDS and FDP need to be visualized from the level of the musculotendinous junction to the level of the entrance into the carpal tunnel. The incision should be extended as necessary to identify the flexor tendons and median nerve (Fig. 24-1).
The FDS and FDP need to be visualized from the level of the musculotendinous junction to the level of the entrance into the carpal tunnel. The incision should be extended as necessary to identify the flexor tendons and median nerve (Fig. 24-1).
 Meticulous hemostasis is necessary with ligation of the small perforating vessels (Fig. 24-2).
Meticulous hemostasis is necessary with ligation of the small perforating vessels (Fig. 24-2).

Procedure
Step 1
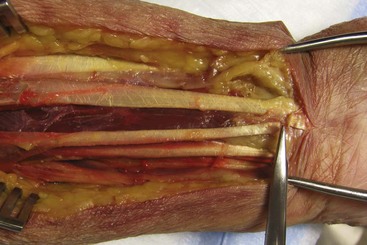
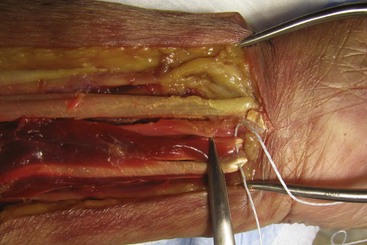
 The palmaris longus is identified, and a tenotomy is performed proximally within the incision. Identify the FDS and FDP tendons, the median nerve as it courses between the FDS and FDP muscle bellies, and the ulnar neurovascular bundle adjacent to the deep FDP muscle belly. Protect these neurovascular structures throughout the tenotomy procedures (Figs. 24-3 and 24-4).
The palmaris longus is identified, and a tenotomy is performed proximally within the incision. Identify the FDS and FDP tendons, the median nerve as it courses between the FDS and FDP muscle bellies, and the ulnar neurovascular bundle adjacent to the deep FDP muscle belly. Protect these neurovascular structures throughout the tenotomy procedures (Figs. 24-3 and 24-4).
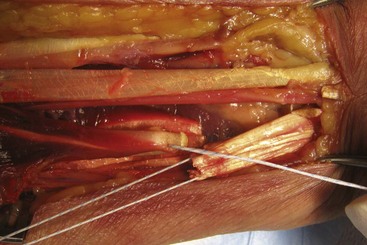
 Just proximal to the transverse carpal ligament, a nonabsorbable suture is placed across the FDS tendons of the index, long, ring, and small fingers in a running, locking manner. This creates a single tendon unit (Fig. 24-5).
Just proximal to the transverse carpal ligament, a nonabsorbable suture is placed across the FDS tendons of the index, long, ring, and small fingers in a running, locking manner. This creates a single tendon unit (Fig. 24-5).
 Wrist flexion facilitates the exposure of the distal FDS tendons.
Wrist flexion facilitates the exposure of the distal FDS tendons.
 The FDS tendons are then sharply transected as distally as possible (Fig. 24-6).
The FDS tendons are then sharply transected as distally as possible (Fig. 24-6).


Step 1 Pearls
Maintain the superficialis tendons in the position of a normal cascade when placing the stay stitch.
Maximum finger flexion delivers the tendons into the surgical field and takes advantage of the full accessible tendon length.
A myotendinous recession or fractional lengthening may be necessary for the FCR and FCU when there is excessive wrist flexion (similar to fractional lengthening of finger flexors described in previous section). Likewise, if there is an excessive forearm pronation contracture, a release of the pronator teres insertion from the radius can be performed.
Step 2




Step 3
 The FDP tendons are then sharply transected as proximally as possible so that the FDS tendons proximally can be transferred to the FDP tendons distally. The muscle of the FDP will now provide the force for the tendons of the FDS.
The FDP tendons are then sharply transected as proximally as possible so that the FDS tendons proximally can be transferred to the FDP tendons distally. The muscle of the FDP will now provide the force for the tendons of the FDS.
 Suture the distal ends of the superficialis tendons to the proximal ends of the profundus tendons while holding the fingers and wrist in a position of maximum extension. Check finger position and evaluate for corrected finger extension and maintenance of normal finger cascade before wound closure (Fig. 24-9).
Suture the distal ends of the superficialis tendons to the proximal ends of the profundus tendons while holding the fingers and wrist in a position of maximum extension. Check finger position and evaluate for corrected finger extension and maintenance of normal finger cascade before wound closure (Fig. 24-9).
 A nonabsorbable, braided suture is used to secure the transfer. Multiple horizontal mattress sutures or a running, locking technique is used (Fig. 24-10).
A nonabsorbable, braided suture is used to secure the transfer. Multiple horizontal mattress sutures or a running, locking technique is used (Fig. 24-10).


Postoperative Care and Expected Outcomes



Braun RM, Vise GT, Roper B. Preliminary experience with superficialis to profundus tendon transfer in the hemiplegic upper extremity. J Bone Joint Surg [Am]. 1974;56:466-472.
Keenan MAE, Korchek JI, Botte MJ, et al. Results of transfer of the flexor digitorum superficialis tendons to the flexor digitorum profundus tendons in adults with acquired spasticity of the hand. J Bone Joint Surg [Am]. 1987;69:1127-1132.


