CHAPTER 23
Medial Epicondylitis
Definition
Epicondylitis is a general term used to describe inflammation, pain, or tenderness in the region of the medial or lateral epicondyle of the humerus. The actual nidus of pain and pathologic change has been debated. Medial epicondylitis implies an inflammatory lesion with degeneration at the origin of the flexor muscles (the medial epicondyle of the humerus). In medial epicondylitis, the tendon of the flexor muscle group is affected (flexor carpi radialis, flexor carpi ulnaris, flexor digitorum superficialis, and palmaris longus).
Although the term epicondylitis implies an inflammatory process, inflammatory cells are not identified histologically. Instead, the condition may be secondary to failure of the musculotendinous attachment with resultant fibroplasia [2], termed tendinosis. Other postulated primary lesions include angiofibroblastic tendinosis, periostitis, and enthesitis [3]. In children, medial elbow pain may result from repetitive stress on the apophysis of the medial epicondyle ossification center (Little Leaguer’s elbow) [4]. Overall, the focus of injury appears to be the muscle origin. Symptoms may be related to failure of the repair process [5].
Repetitive stress has been implicated as a factor in this condition [6]. Poor throwing mechanics and excessive throwing have been implicated in Little Leaguer’s elbow. Repetitive wrist flexion, as in the trailing arm in a golf swing, can cause medial epicondylitis (hence, the term golfer’s elbow is frequently used for medial epicondylitis, regardless of etiology).
Symptoms
Patients usually report pain in the area just distal to the medial epicondyle. The patient may complain of pain radiating proximally or distally. Patients may also complain of pain with wrist or hand movement, such as gripping a doorknob, carrying a briefcase, or shaking hands. Patients occasionally report swelling as well.
Physical Examination
On examination, the hallmark of epicondylitis is tenderness over the flexor muscle origin (medial epicondylitis). The origin of the flexor muscles can be located one fingerbreadth below the medial epicondyle. With medial epicondylitis, pain is increased with resisted wrist flexion. There may be localized tenderness along the course of the radial nerve around the radial head. Motor and sensory findings are usually absent.
Functional Limitations
The patient may complain of an inability to lift or to carry objects on the affected side secondary to increased pain. Typing, using a computer mouse, or working on a keyboard may re-create the pain. Even handshaking or hand squeezing may be painful in medial epicondylitis. Athletic activities may cause pain, especially with an acute increase in repetition, poor technique, and equipment changes.
Diagnostic Studies
The diagnosis is usually made on clinical grounds. Magnetic resonance imaging, which is particularly useful for soft tissue definition, can be used to assess for tendinitis, tendinosis, degeneration, partial tears or complete tears, and detachment of the common flexor at the medial epicondyles [7]. Magnetic resonance imaging is rarely needed, however, except in recalcitrant epicondylitis, and it will not alter the treatment significantly in the early stages. The medial collateral ligament complexes can be evaluated for tears as well as for chronic degeneration and scarring. Ultrasonography has been used to diagnose medial epicondylitis [8,9]. Arthrography may be beneficial if capsular defects and associated ligament injuries are suspected. Barring evidence of trauma, early radiographs are of little help in this condition but may be useful in cases of resistant tendinitis and to rule out occult fractures, arthritis, and osteochondral loose body. Early radiographic studies (before commencing a rehabilitation program) may be considered in skeletally immature children with elbow pain to rule out growth plate disorders, osteochondritis dissecans, or ulnar collateral ligament tears [10].
Treatment
Initial
Initial treatment consists of relative rest, avoidance of repetitive motions involving the wrist, activity modification to avoid stress on the epicondyle, anti-inflammatory medications, and thermal modalities such as heat and ice for acute pain. Patients who develop medial epicondylitis from golf should consider modifying their swing to avoid excessive force on wrist flexor muscles. Biomechanical modifications may help reduce symptoms if the medial epicondylitis is thought to be due to poor pitching technique.
In addition, a forearm band (counterforce brace) worn distal to the flexor muscle group origin can be beneficial. The theory behind this device is that it will dissipate forces over a larger area of tissue than the medial attachment site [15]. Alternatively, the use of wrist immobilization splints may be helpful. A splint set in neutral can be helpful for medial epicondylitis by relieving the tension on the flexors and extensors of the wrist and fingers. Dynamic extension bracing has also been proposed [16].
Rehabilitation
Rehabilitation may include physical or occupational therapy. Therapy should include two phases. The first phase is directed at decreasing pain by physical modalities (ultrasound, electrical stimulation, phonophoresis, heat, ice, massage) and decreasing disability (education, reduction of repetitive stress, and preservation of motion). When the patient is pain free, a gradual program is implemented to improve strength and endurance of wrist flexors and should include stretching. This program must be carefully monitored to permit strengthening of the muscles and work hardening of the tissues without itself causing an overuse situation. The patient should start with static exercises and advance to progressive resistive exercises. Thera-Band, light weights, Kinesio taping [17], and manual (self) resistance exercises can be used.
Work or activity restrictions or modifications may be required for a time.
Procedures
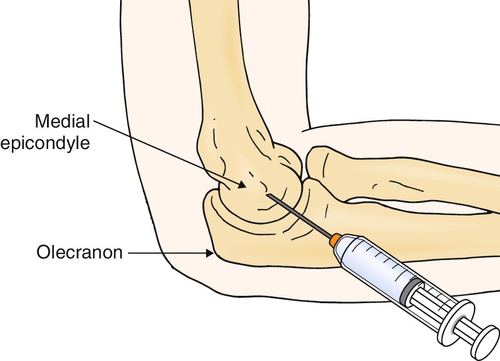
Injection of corticosteroid, usually with a local anesthetic, into the area of maximum tenderness (approximately 1 to 5 cm distal to the medial epicondyle) has been shown to be effective in treatment of epicondylitis (Fig. 23.1) [18,19]. To confirm the diagnosis, a trial of lidocaine alone may be given. An immediate improvement in grip strength should be noted after injection. Postinjection treatment includes icing of the affected area both immediately (for 5 to 10 minutes) and thereafter (a reasonable regimen is 20 minutes two or three times per day for 2 weeks) and wearing of a wrist splint (particularly for activities that involve wrist movement). The wrist splint should be set in neutral for medial epicondylitis. Exacerbating activities are to be avoided. Platelet-rich plasma injections have been shown to reduce pain and to increase function in patients with recalcitrant epicondylitis [20], as have botulinum toxin injections [21].
Injections for medial epicondylitis must be used cautiously because of the risk of injury to the ulnar nerve (either by direct injection or by tissue changes that may promote nerve injury).
Surgery
Surgery may be indicated in those patients with continued severe symptoms who do not respond to conservative management. Surgery is aimed at excision and revitalization of the pathologic tissue and release of the muscle origin [22]. Pinning may be done if the elbow joint is unstable [4].
Potential Disease Complications
Possible long-term complications of untreated epicondylitis include chronic pain, loss of function, and possible elbow contracture. Medial epicondylitis may lead to reversible impairment (neurapraxia) of the ulnar nerve [23]. In general, epicondylitis is more easily and successfully treated in the acute phase.
Potential Treatment Complications
Analgesics and nonsteroidal anti-inflammatory drugs have well-known side effects that most commonly affect the gastric, hepatic, and renal systems. Local steroid injections may increase the risk for disruption of tissue planes, create high-pressure tissue necrosis, rupture tendons [1], damage nerves, promote skin depigmentation or atrophy, or cause infection [24].






