Procedure 23 Fractional Lengthening of the Flexor Tendons
 See Video 20: Fractional Lengthening of the Flexor Tendons
See Video 20: Fractional Lengthening of the Flexor Tendons
Indications



Examination/Imaging






Surgical Anatomy
 Pertinent surgical anatomy includes the volar forearm muscles (palmaris longus, flexor carpi radialis, flexor carpi ulnaris, flexor digitorum superficialis, FDP, pronator teres, pronator quadratus), median nerve, ulnar nerve and artery, and radial artery. Cross-sectional anatomy should be reviewed before intervention.
Pertinent surgical anatomy includes the volar forearm muscles (palmaris longus, flexor carpi radialis, flexor carpi ulnaris, flexor digitorum superficialis, FDP, pronator teres, pronator quadratus), median nerve, ulnar nerve and artery, and radial artery. Cross-sectional anatomy should be reviewed before intervention.


Exposures
 A longitudinal volar incision over the junction of the mid to distal third of the forearm is used. This corresponds to the myotendinous junction of the volar flexor musculature.
A longitudinal volar incision over the junction of the mid to distal third of the forearm is used. This corresponds to the myotendinous junction of the volar flexor musculature.
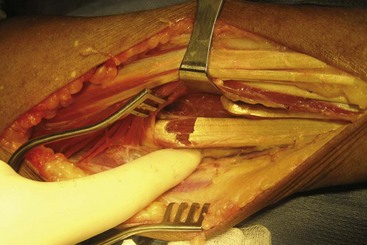
 Division of the volar forearm fascia exposes the underlying musculotendinous junctions (Fig. 23-1).
Division of the volar forearm fascia exposes the underlying musculotendinous junctions (Fig. 23-1).
 Cutaneous volar veins should be mobilized and ligated as necessary.
Cutaneous volar veins should be mobilized and ligated as necessary.
Pearls
The ulnar nerve is more volar and ulnar than the ulnar artery. The FDP tendons are supplied by segmental arterioles from the ulnar artery. Hemostasis of these vessels is important in preventing postoperative hematoma.
Identify the median nerve before any musculotendinous recessions. It can be difficult to differentiate the median nerve from the finger flexor tendons, especially under tourniquet application. The vascularity of the nerve is different from the tendon. The nerve is typically supplied by longitudinal vessels. One cannot rely on the tension of the structures in these severe contracture situations.
Procedure
Step 1
 The tendinous portion of the myotendinous structure is identified, carefully verifying that the muscular portion is in continuity. The tendon is then identified into the distal muscle belly, without disturbing the muscle fibers (Fig. 23-2).
The tendinous portion of the myotendinous structure is identified, carefully verifying that the muscular portion is in continuity. The tendon is then identified into the distal muscle belly, without disturbing the muscle fibers (Fig. 23-2).


Step 2
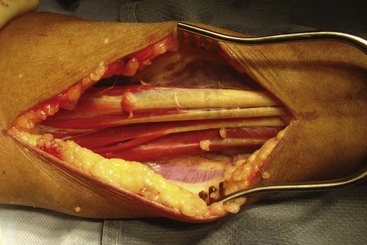
 A sharp tendon division is made at the musculotendinous junction in each flexor digitorum superficialis tendon (Fig. 23-3).
A sharp tendon division is made at the musculotendinous junction in each flexor digitorum superficialis tendon (Fig. 23-3).
 Each digit is passively stretched into extension, allowing the tendon and muscle fibers to slide distally. A 2- to 3-cm gap between the two ends of the tendon will be visualized (Fig. 23-4).
Each digit is passively stretched into extension, allowing the tendon and muscle fibers to slide distally. A 2- to 3-cm gap between the two ends of the tendon will be visualized (Fig. 23-4).

Step 3
 Once all flexor digitorum superficialis tendons are lengthened appropriately, lengthening of the FDP tendons is usually necessary to obtain better digital extension. The examination under anesthesia is helpful in determining the preoperative need to lengthen the FDS and FDP.
Once all flexor digitorum superficialis tendons are lengthened appropriately, lengthening of the FDP tendons is usually necessary to obtain better digital extension. The examination under anesthesia is helpful in determining the preoperative need to lengthen the FDS and FDP.
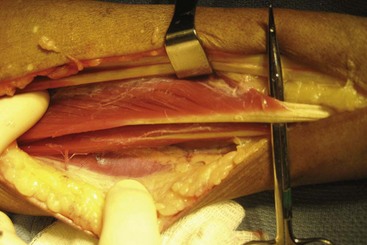
 Meticulous dissection deep to the FDP tendons includes hemostasis of segmental arterioles from the ulnar artery (Fig. 23-5).
Meticulous dissection deep to the FDP tendons includes hemostasis of segmental arterioles from the ulnar artery (Fig. 23-5).
 The FDP tendons are completely visualized and isolated for lengthening (Fig. 23-6).
The FDP tendons are completely visualized and isolated for lengthening (Fig. 23-6).
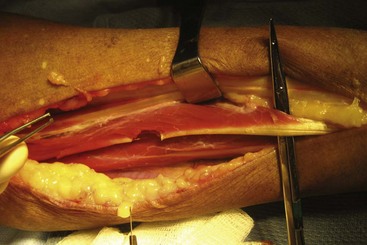
 A similar tendon division is made at the musculotendinous junction of each FDP tendon (Fig. 23-7).
A similar tendon division is made at the musculotendinous junction of each FDP tendon (Fig. 23-7).