Procedure 22 Intrinsic Muscle Release for Thumb-in-Palm Deformity
 See Video 19: Intrinsic Muscle Release for Thumb-in-Palm Deformity and Adductor Release Using a Thenar Incision
See Video 19: Intrinsic Muscle Release for Thumb-in-Palm Deformity and Adductor Release Using a Thenar IncisionIndications



Examination/Imaging











Exposures
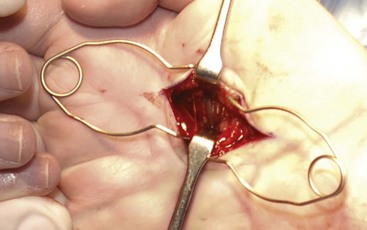
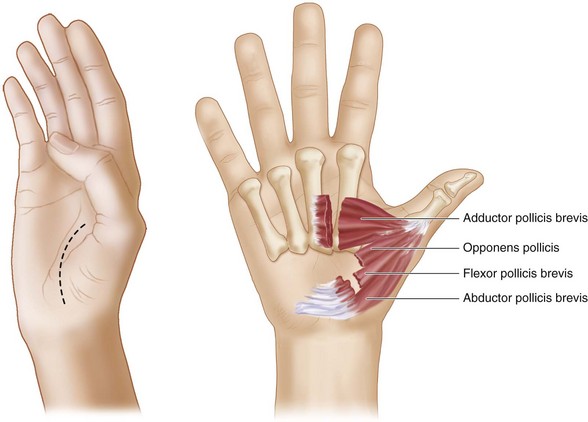
 A palmar incision is made paralleling the thenar crease (Fig. 22-4).
A palmar incision is made paralleling the thenar crease (Fig. 22-4).

 Identify the lumbrical muscle and common digital artery and nerve.
Identify the lumbrical muscle and common digital artery and nerve.
 Gently retract the lumbrical muscle and the neurovascular bundle ulnarly to visualize the enveloping thumb adductor muscle fascia. The thumb adductor muscle, with transverse muscle fibers beneath, originates on the radial side of the long finger metacarpal (Fig. 22-5).
Gently retract the lumbrical muscle and the neurovascular bundle ulnarly to visualize the enveloping thumb adductor muscle fascia. The thumb adductor muscle, with transverse muscle fibers beneath, originates on the radial side of the long finger metacarpal (Fig. 22-5).

Procedure
Step 1


Step 2
 If necessary, proceed to release of thenar muscle contracture.
If necessary, proceed to release of thenar muscle contracture.
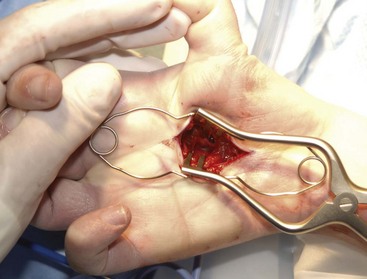
 Origins of both heads of flexor pollicis brevis, opponens pollicis, and abductor pollicis brevis muscles are identified on the volar carpal ligament and sharply sectioned with care (Fig. 22-7).
Origins of both heads of flexor pollicis brevis, opponens pollicis, and abductor pollicis brevis muscles are identified on the volar carpal ligament and sharply sectioned with care (Fig. 22-7).
 Again, passively abduct and extend the thumb, allowing the muscles to retract.
Again, passively abduct and extend the thumb, allowing the muscles to retract.
Step 2 Pearls
Preserve the motor branch of the median nerve to the thenar muscles.
The first dorsal interosseous muscle can be released from the thumb metacarpal base if residual contracture remains; however, this is usually not necessary.
Pin the thumb metacarpal in abduction with smooth K-wires if tightness persists.





