Procedure 21 Steindler Flexorplasty
Indications
 Late presentation of upper trunk brachial plexus palsy (C5-C6; C5-C6-C7) without recovery of elbow flexion.
Late presentation of upper trunk brachial plexus palsy (C5-C6; C5-C6-C7) without recovery of elbow flexion.

Examination/Imaging




Surgical Anatomy
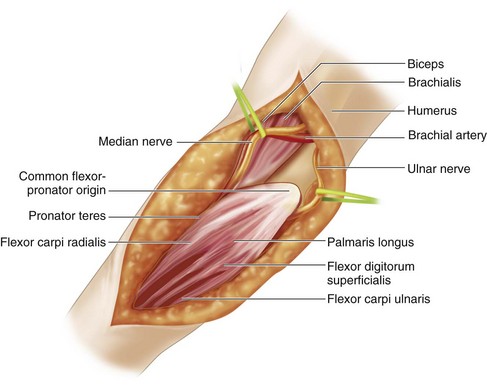
 The common flexor-pronator muscles originate from the medial epicondyle. The following muscles are elevated during this procedure: pronator teres, FCR, palmaris longus, FCU, and flexor digitorum superficialis (Fig. 21-1). The flexor digitorum profundus is left in situ (see Fig. 21-1).
The common flexor-pronator muscles originate from the medial epicondyle. The following muscles are elevated during this procedure: pronator teres, FCR, palmaris longus, FCU, and flexor digitorum superficialis (Fig. 21-1). The flexor digitorum profundus is left in situ (see Fig. 21-1).

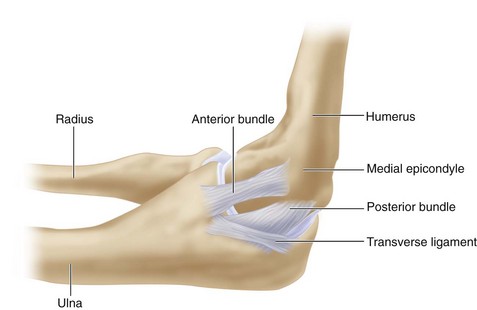
 The medial (ulnar) collateral ligament of the elbow should be protected during elevation of the flexor-pronator mass. It originates at the posterior distal aspect of the medial epicondyle and inserts into the base of the coronoid process of ulna. It is composed of three bands: anterior, posterior, and transverse (Fig. 21-2).
The medial (ulnar) collateral ligament of the elbow should be protected during elevation of the flexor-pronator mass. It originates at the posterior distal aspect of the medial epicondyle and inserts into the base of the coronoid process of ulna. It is composed of three bands: anterior, posterior, and transverse (Fig. 21-2).

Exposures
 A 10-cm longitudinal curvilinear incision centered over the medial epicondyle is made (Fig. 21-3).
A 10-cm longitudinal curvilinear incision centered over the medial epicondyle is made (Fig. 21-3).
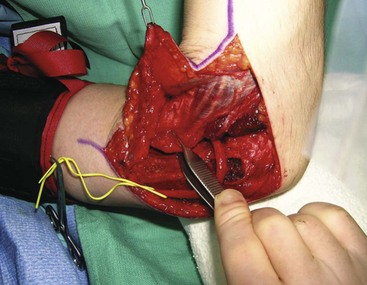
 A skin flap is elevated while protecting the medial antebrachial cutaneous nerve. After elevation of the skin flap, one will see the flexor-pronator mass attaching to the medial epicondyle (Fig. 21-4).
A skin flap is elevated while protecting the medial antebrachial cutaneous nerve. After elevation of the skin flap, one will see the flexor-pronator mass attaching to the medial epicondyle (Fig. 21-4).
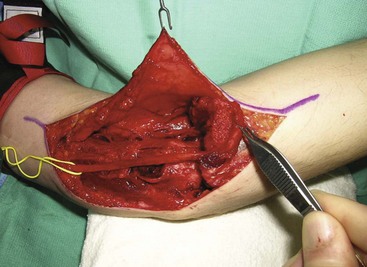
 The ulnar nerve is protected, and a vessel loop is placed around the nerve for identification and gentle traction (Fig. 21-5).
The ulnar nerve is protected, and a vessel loop is placed around the nerve for identification and gentle traction (Fig. 21-5).
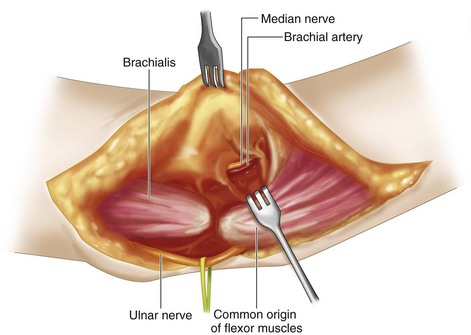
 Lateral to the flexor-pronator mass, the brachial artery and median nerve are seen entering the arch over the superficialis muscles (Fig. 21-6).
Lateral to the flexor-pronator mass, the brachial artery and median nerve are seen entering the arch over the superficialis muscles (Fig. 21-6).



Procedure
Step 1
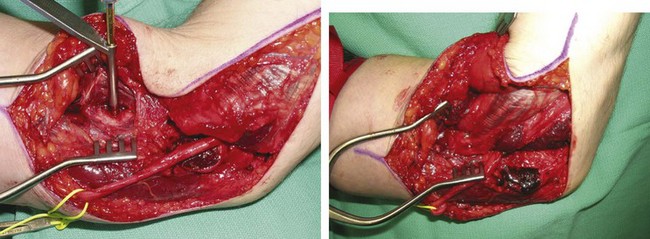
 The index finger is placed under the flexor-pronator mass to develop an interval plane between the median nerve and the entire flexor-pronator mass (Fig. 21-7). The ulnar head of FCU is dissected from the ulna.
The index finger is placed under the flexor-pronator mass to develop an interval plane between the median nerve and the entire flexor-pronator mass (Fig. 21-7). The ulnar head of FCU is dissected from the ulna.

Step 2


Step 4

Step 5
 The medial epicondyle can be provisionally fixed to the trough created in the distal humerus and secured using a towel clip.
The medial epicondyle can be provisionally fixed to the trough created in the distal humerus and secured using a towel clip.
 Secure fixation to the humerus is achieved by passing a 3.5-mm cortical screw over a washer through the medial epicondyle. A 2.5-mm drill bit and a 3.5-mm tap are used for this purpose (Fig. 21-11).
Secure fixation to the humerus is achieved by passing a 3.5-mm cortical screw over a washer through the medial epicondyle. A 2.5-mm drill bit and a 3.5-mm tap are used for this purpose (Fig. 21-11).

Postoperative Care and Expected Outcomes
 The elbow is splinted at 90 degrees for 6 weeks to allow fusion of the osteotomized medial epicondyle to the humerus. After 2 weeks, the sutures are removed, and a thermoplastic splint is made to immobilize the elbow at 90 degrees of flexion for another 4 weeks. During the first 6 weeks, the patient should move the fingers to prevent contracture. After 6 weeks, the patient is started on gentle gravity-assisted extension of the elbow while initiating elbow flexion exercises. After 12 weeks, resisted flexion is started.
The elbow is splinted at 90 degrees for 6 weeks to allow fusion of the osteotomized medial epicondyle to the humerus. After 2 weeks, the sutures are removed, and a thermoplastic splint is made to immobilize the elbow at 90 degrees of flexion for another 4 weeks. During the first 6 weeks, the patient should move the fingers to prevent contracture. After 6 weeks, the patient is started on gentle gravity-assisted extension of the elbow while initiating elbow flexion exercises. After 12 weeks, resisted flexion is started.

Chen WS. Restoration of elbow flexion by modified Steindler flexorplasty. Int Orthop. 2000;24:43-46.
Dutton RO, Dawson EG. Elbow flexorplasty: an analysis of long-term results. J Bone Joint Surg [Am]. 1981;63:1064-1069.
Goldfarb CA, Burke MS, Manske PR, et al. The Steindler flexorplasty for the arthrogrypotic elbow. J Hand Surg [Am]. 2004;29:462-469.
Liu TK, Yang RS, Sun JS. Long-term results of the Steindler flexorplasty. Clin Orthop Relat Res. 1993;296:104-108.
Monreal R. Steindler flexorplasty to restore elbow flexion in C5-C6-C7 brachial plexus palsy type. J Brachial Plex Peripher Nerve Inj. 2007;2:15.


