CHAPTER 21 Mechanical Ventilation in Critical Illness
1 Why might a patient require mechanical ventilation?
There are three conditions for which mechanical ventilation (MV) may be required:










11 What are trigger variables?
All modern ICU ventilators constantly measure one or more of the phase variables (i.e., pressure, volume, flow, or time) (Table 21-1). Inspiration occurs when one of these variables reaches a preset value. Clinically this is referred to as triggering the ventilator. The following conditions are necessary to initiate a breath under each individual variable:
 Pressure triggering: requires patient-initiated effort to decrease circuit pressure below a preset value (e.g., −2 cm H2O below baseline end-expiratory pressure is common).
Pressure triggering: requires patient-initiated effort to decrease circuit pressure below a preset value (e.g., −2 cm H2O below baseline end-expiratory pressure is common).

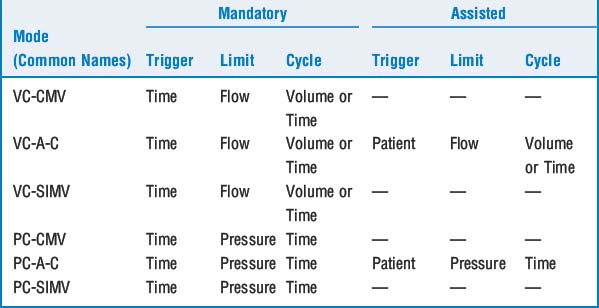
Two potentially hazardous forms of triggering have also been identified:
 Auto-triggering: occurs when the ventilator is rapidly cycling without apparent patient effort. If the triggering system is overly sensitive (e.g., the pressure is set for −1 cm H2O) and excessive condensation is present within the circuit, water motion can result in a drop in circuit pressure, causing auto-cycling.
Auto-triggering: occurs when the ventilator is rapidly cycling without apparent patient effort. If the triggering system is overly sensitive (e.g., the pressure is set for −1 cm H2O) and excessive condensation is present within the circuit, water motion can result in a drop in circuit pressure, causing auto-cycling.
14 What is the role of positive end-expiratory pressure?



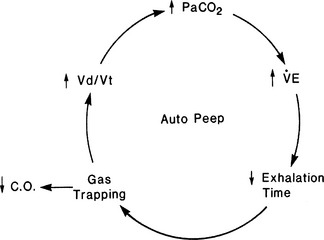
16 What is intrinsic or auto-positive end-expiratory pressure?
Failure to recognize the presence of auto-PEEP can lead to inappropriate ventilator changes (Figure 21-1). The only way to detect and measure PEEPi is to occlude the expiratory port at end expiration while monitoring airway pressure. Decreasing rate or increasing inspiratory flow (to increase I:E ratio) may allow time for full exhalation. Administering a bronchodilator therapy in the setting of bronchospasm is usually beneficial.














26 How is the patient who is fighting the ventilator approached?
KEY POINTS: Mechanical Ventilation in Critical Illness 

1. Alsaghir A.H., Martin C.M. Effects of prone positioning in patients with acute respiratory distress syndrome: a meta-analysis. Crit Care Med. 2008;36:603-609.
2. Fessler H.E., Hess D.R. Does high-frequency ventilation offer benefits over conventional ventilation in adult patients with acute respiratory distress syndrome? Respir Care. 2007;52:595-608.
3. Kallet R.H., Branson R.D. Do the NIH ARDS Clinical Trials Network PEEP/FIO2 tables provide the best evidence-based guide to balancing PEEP and FIO2 settings in adults? Respir Care. 2007;52:461-477.
4. MacIntyre N.R. Is there a best way to set tidal volume for mechanical ventilatory support? Clin Chest Med. 2008;29:225-231.
5. Nichols D., Haranath S. Pressure control ventilation. Crit Care Clin. 2007;23:183-199.
6. Steinburg K.P., Kacmarek R.M. Should tidal volume be 6 mL/kg predicted body weight in virtually all patients with acute respiratory failure? Respir Care. 2007;52:556-567.
