Cytoplasmic Pigment H&E at high power shows lipofuscin pigment in centrizonal hepatocytes.
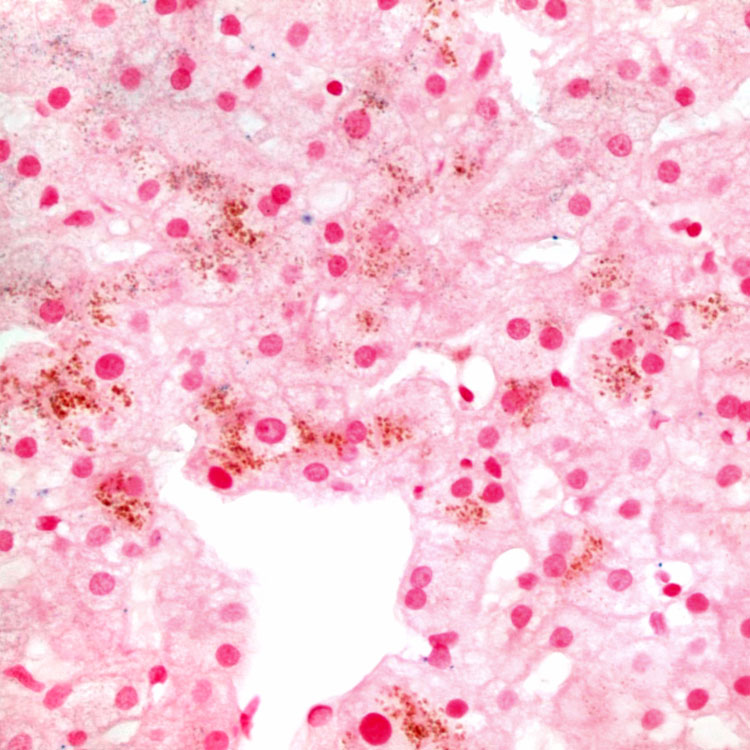
PAS-D Stain Periodic acid-Schiff with diastase digestion accentuates the granular pigment in centrizonal hepatocytes , even though the pigment is not PAS-D positive.
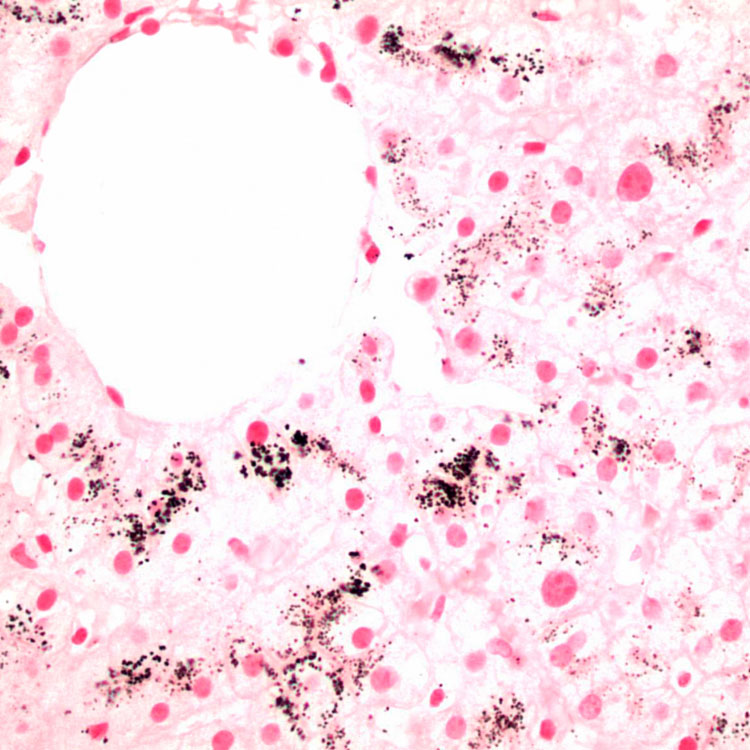
Fontana-Masson Stain Fontana-Masson stain highlights the increased lipofuscin marked by black staining in the centrizonal hepatocytes.
Iron Stain Prussian blue stain for iron is negative and helps to confirm that the cytoplasmic pigment is not hemosiderin.
TERMINOLOGY
Definitions
• Inherited unconjugated hyperbilirubinemia due to mutations of bilirubin uridine diphosphate glucuronosyltransferase (B-UGT or UGT1A1 ) gene
ETIOLOGY/PATHOGENESIS
Genetic Disorder
• Extra TA in TATAA box of UGT1A1 promoter (this variant is known as B-UGT*28)
Decreased transcription of gene to 20% of normal
– Decreased conjugation of bilirubin with glucuronic acid
– Decreased conjugation of some drugs (irinotecan, atazanavir, TAS-103, indinavir, tolbutamide, rifamycin)
• Affected patients typically have 2nd condition causing increased bilirubin load
Examples of additional condition include reduced red blood cell lifespan or impaired hepatic bilirubin uptake
CLINICAL ISSUES
Epidemiology
• Incidence
Among Caucasians, mutation has frequency of 35-40%
– 11-16% of population homozygous
• Age
Often diagnosed at puberty, possibly related to increased hemoglobin turnover and inhibition of bilirubin glucuronidation by endogenous steroid hormones
[level-membership-for-pathology-category]
• Sex
Males affected more than females, possible due to higher rate of bilirubin production in males
Presentation
• Mild unconjugated nonhemolytic hyperbilirubinemia, usually fluctuating and < 3 mg/dL
• Higher bilirubin can occur during illness, stress, or menstrual period
• Otherwise normal liver function
• Jaundice is only finding on physical examination
• Associated with prolonged neonatal jaundice and development of gallstones in patients with hereditary spherocytosis
• Associated with increased risk of toxicity from drugs metabolized by B-UGT
Irinotecan has been associated with severe diarrhea and neutropenia
Increased risk of hyperbilirubinemia with atazanavir
Laboratory Tests
• Mild unconjugated hyperbilirubinemia
• Normal alkaline phosphatase, aspartate aminotransferase, alanine aminotransferase, γ-glutamyl transpeptidase
• Increased proportion of bilirubin monoglucuronide in bile
• Rifampin administration causes disproportionate unconjugated hyperbilirubinemia relative to normal patients
• Caloric restriction causes disproportionate unconjugated hyperbilirubinemia relative to normal patients
Treatment
• No treatment necessary
Prognosis
• Excellent
MACROSCOPIC
General Features
• No macroscopic findings
MICROSCOPIC
Histologic Features
• Increased lipofuscin in centrizonal hepatocytes
Predominant Pattern/Injury Type
• Pigment accumulation
Predominant Cell/Compartment Type
• Hepatocyte
DIFFERENTIAL DIAGNOSIS
Lipofuscin Deposition
• Increased lipofuscin can be seen in advancing age, chronic drug ingestion, and as variant of normal
Dubin-Johnson Syndrome
• Pigment is considerably more coarse
Crigler-Najjar, Types 1 and 2
• Severe unconjugated hyperbilirubinemia characterized by total or near-total absence of B-UGT activity
• Mutations in exons 1-5 of UGT1A1 gene
• Biopsy can show cholestasis or appear normal
DIAGNOSTIC CHECKLIST
Clinically Relevant Pathologic Features
• Does not lead to liver inflammation, fibrosis, cirrhosis, or liver failure
• Testing for B-UGT*28 often done to identify patients at risk for certain drug toxicities and to tailor dose
 in centrizonal hepatocytes.
in centrizonal hepatocytes.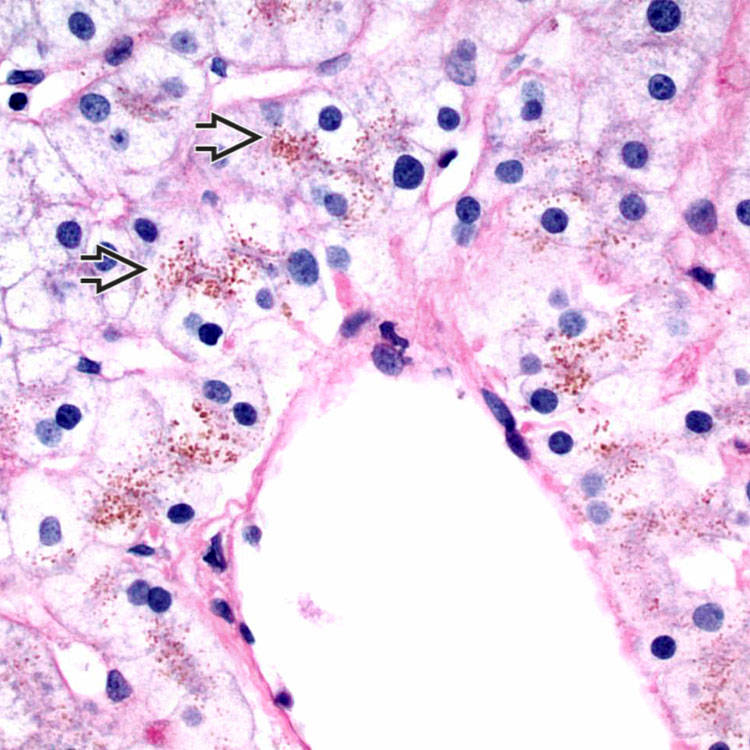
 , even though the pigment is not PAS-D positive.
, even though the pigment is not PAS-D positive.