Lab data: Increased WBC and ESR; positive fecal occult blood test
• Treatment: Colectomy and treatment of complications
• Prognosis: Good following colectomy without perforation
Poor if colonic perforation and sepsis precede colectomy
• Seen in ∼ 5% of infectious or ulcerative colitis patients
DIAGNOSTIC CHECKLIST
• Consider prior history of infectious or ulcerative colitis
• Dilated colon with air-fluid levels; thickened or absent transverse folds in a very sick patient
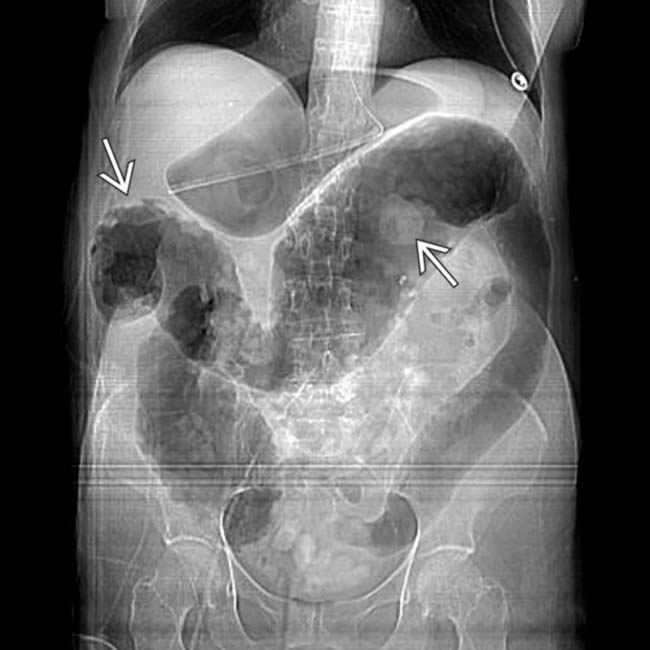
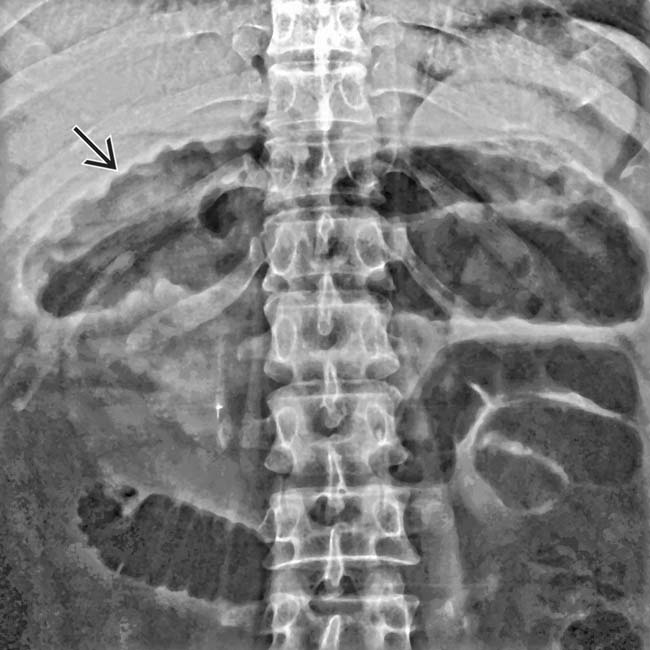
(Left) Supine radiograph in a 58-year-old woman, who presented with severe abdominal pain and bloody diarrhea, illustrates the typical appearance of toxic megacolon on plain film. The transverse colon is dilated with marked thickening of the transverse folds .
(Right) This 35-year-old man with a history of ulcerative colitis presents with acute severe abdominal pain and distention. This supine radiograph shows a dilated, ahaustral transverse colon with a “shaggy” surface contour.
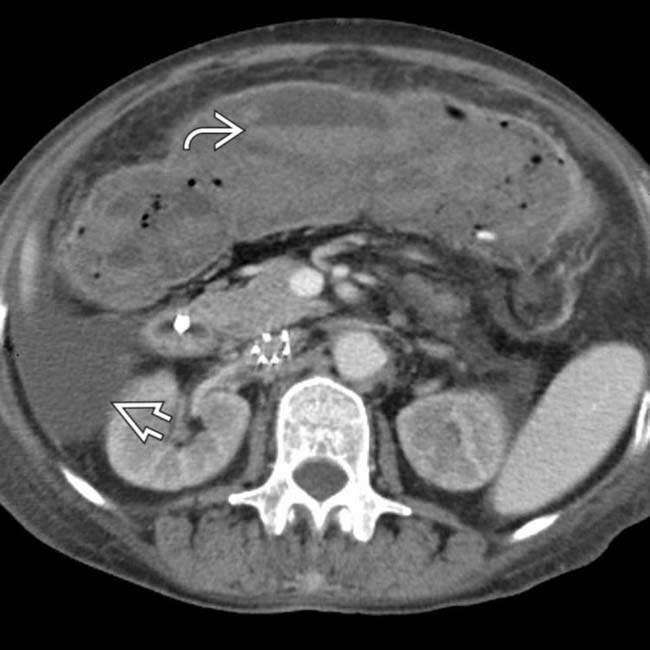
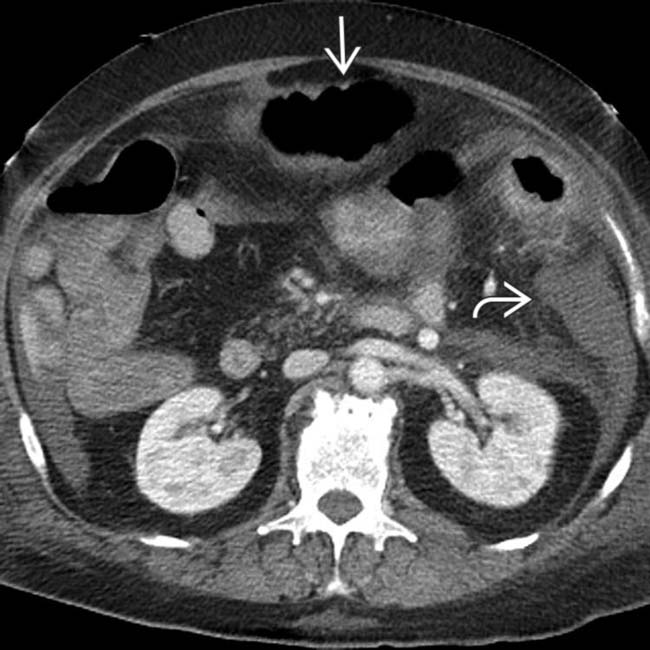
(Left) This woman developed Clostridium difficile colitis while hospitalized for other reasons. CT shows ascites , marked dilation of the colon with loss of transverse folds, and intraluminal high-density material representing hemorrhage and sloughed mucosa.
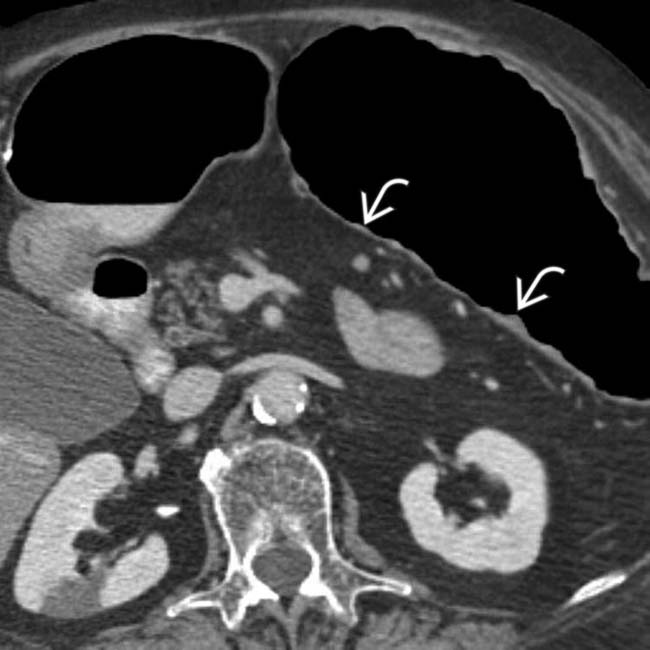
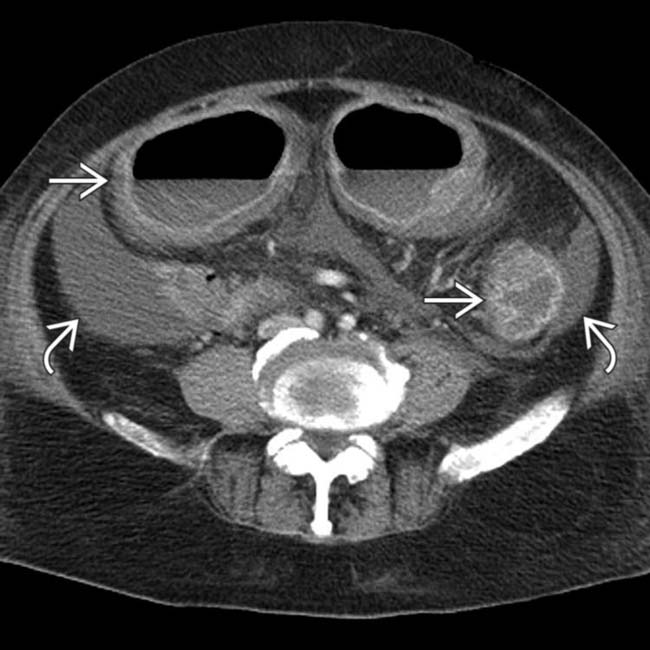
(Right) Axial CECT in the same case shows a generalized ileus . The colon is massively distended with blood and debris and its wall is relatively thin. Soon after this scan, the colon perforated and a total colectomy was required.
TERMINOLOGY
Definitions
• Acute transmural fulminant colitis with neuromuscular degeneration and colonic dilation
IMAGING
General Features
• Best diagnostic clue
Dilated ahaustral colon with pseudopolyps and air-fluid levels
• Location
Transverse colon > other segments
Radiographic Findings
• Radiography
Hallmark: Marked colonic dilatation with abnormal or absent fold pattern
– Transverse colon most common ± other segments
– Increased colon caliber on serial radiographs
> 5 cm on CT, often > 8 cm (as measured on supine radiograph)
– Transverse colonic folds may be thickened (edema or hemorrhage), or lost (sloughed mucosa and submucosa)
– Mucosal islands or pseudopolyps cause irregular surface contour
– Pneumatosis coli ± pneumoperitoneum
CT Findings
• Colon distended with gas, fluid ± blood
• Distorted or absent transverse fold pattern
• Irregular nodular contour of colonic wall (mucosal pseudopolyps)
• ± intramural gas ± blood
• ± free intraperitoneal gas and fluid
Imaging Recommendations
• Best imaging tool
CECT with multiplanar reformations
DIFFERENTIAL DIAGNOSIS
Colonic Obstruction
• Gas- and stool-filled colon to point of obstruction
• Retained transverse fold and mucosal patterns excludes toxic megacolon
Adynamic or Paralytic Ileus
• Dilated small and large bowel without transition point
• Normal transverse fold pattern excludes toxic megacolon
PATHOLOGY
General Features
• Etiology
Clostridium difficile and other infectious colitis
– Now the most common etiology
– Ulcerative (and granulomatous) colitis had been more common in past
Amebiasis, strongyloidiasis, bacillary dysentery
Typhoid fever, cholera, Behçet syndrome
Gross Pathologic & Surgical Features
• Colon is grossly dilated with fluid and gas
• Wall may appear thinned or thick
• Hemorrhagic necrosis of colonic mucosa and submucosa
Seen in ∼ 5% of patients with infectious or ulcerative colitis
– Medical and surgical mortality: > 20%
– Most severe, life-threatening complication of colitis
Natural History & Prognosis
• For infectious colitis
Delayed diagnosis or failed antibiotic therapy may result in toxic megacolon
• For ulcerative colitis, predisposing factors
Endoscopy; use of opiates and anticholinergic drugs
• Complications: Perforation, peritonitis, death
• Prognosis: Good following colectomy without perforation
Poor if colonic perforation and sepsis precede colectomy
Treatment
• Colectomy; treat complications
DIAGNOSTIC CHECKLIST
Consider
• Prior history of infectious or ulcerative colitis
Image Interpretation Pearls
• Dilated colon with air-fluid levels; thickened or absent transverse folds in a very sick patient
(Left) This 68-year-old woman has longstanding Crohn (granulomatous) colitis with acute exacerbation. This supine film shows marked dilation of the transverse colon with a featureless ahaustral appearance. There is some irregularity of the luminal surface , suggesting mucosal sloughing or pseudopolyps.
(Right) Axial CECT in the same patient shows the colonic dilation and ahaustral appearance with marked thinning of the wall, which suggests a risk of perforation.
(Left) A magnified view of the same CT section shows tags of inflamed mucosa or pseudopolyps within the dilated, thin-walled transverse colon.
(Right) Another CT section in the same patient shows fluid , distention and thinning of the walls of the colon, as well as more mucosal pseudopolyps .
(Left) Axial CECT in the same patient shows similar involvement of the rectosigmoid colon . Because of symptoms that were refractory to medical management, as well as these CT findings, the patient had a total colectomy.
(Right) Gross pathology photograph from a similar patient who underwent colectomy illustrates hemorrhagic necrosis of the colonic mucosa and pseudopolyps in a case of toxic megacolon.
(Left) This 61-year-old man was hospitalized for unrelated reasons and developed acute pain, diarrhea, hypotension, and tachycardia. This supine film shows bulging flanks due to ascites. The colon is diffusely dilated with a loss of the normal transverse fold pattern. The folds that are seen are grossly thickened and have a “thumbprint” appearance .
(Right) Axial CECT in the same patient shows ascites and colonic distension .
(Left) Another CT section in the same patient shows that the colon is distended with gas and fluid to a diameter of 7 cm. The mucosa is hyperenhancing and the wall is thickened by submucosal edema . No normal transverse folds are evident. Ascites fills the paracolic gutters , accounting for the bulging flanks seen on plain films.
(Right) Pelvic CT section in the same patient shows marked fluid distention and wall thickening of the rectosigmoid colon .
(Left) Coronal reformatted CT section in the same patient shows the markedly distended sigmoid colon with a complete loss of its normal transverse fold pattern.
(Right) Another CT section in the same patient confirms the pancolitis and ascites . These CT and clinical features are classic for toxic megacolon due to infectious colitis (C. difficile), confirmed at urgent colectomy. The colonic mucosa showed extensive necrosis and sloughing, but no frank perforation was found.
Anteroposterior radiograph shows the typical appearance of toxic megacolon with diffuse colonic distention, especially transverse and descending, and the suggestion of wall thickening due to subserosal and omental edema.
Anteroposterior radiograph shows severe and classic toxic megacolon. Note the colonic distention, especially transverse, and the suggestion of pseudopolyps .
Anteroposterior CECT demonstrates the typical appearance of toxic megacolon on plain film. Note the diffuse colonic dilatation with marked thumbprinting .
Anteroposterior radiograph of supine abdomen demonstrates marked dilatation of transverse colon with a scalloped contour indicating edematous mucosa.
Anteroposterior radiograph of transverse colon in a patient with ulcerative colitis shows a variant appearance of toxic megacolon. The colon is ahaustral but without pseudopolyps typically seen in toxic megacolon.
Supine radiograph shows diffusely dilated bowel in an acutely ill patient with ulcerative colitis. The transverse colon is dilated and ahaustral with an irregular mucosal surface.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Transverse colonic folds may be thickened (edema or hemorrhage), or lost (sloughed mucosa and submucosa)
TOP DIFFERENTIAL DIAGNOSES
• Colonic obstruction or Ileus
Preservation of mucosal and transverse fold pattern
PATHOLOGY
• Clostridium difficile and other infectious colitis
Now the most common etiology
Ulcerative colitis was more common in past
CLINICAL ISSUES
• Most severe, life-threatening complication of colitis
Lab data: Increased WBC and ESR; positive fecal occult blood test
• Treatment: Colectomy and treatment of complications
• Prognosis: Good following colectomy without perforation
Poor if colonic perforation and sepsis precede colectomy
• Seen in ∼ 5% of infectious or ulcerative colitis patients
DIAGNOSTIC CHECKLIST
• Consider prior history of infectious or ulcerative colitis
• Dilated colon with air-fluid levels; thickened or absent transverse folds in a very sick patient
(Left) Supine radiograph in a 58-year-old woman, who presented with severe abdominal pain and bloody diarrhea, illustrates the typical appearance of toxic megacolon on plain film. The transverse colon is dilated with marked thickening of the transverse folds .
(Right) This 35-year-old man with a history of ulcerative colitis presents with acute severe abdominal pain and distention. This supine radiograph shows a dilated, ahaustral transverse colon with a “shaggy” surface contour.
(Left) This woman developed Clostridium difficile colitis while hospitalized for other reasons. CT shows ascites , marked dilation of the colon with loss of transverse folds, and intraluminal high-density material representing hemorrhage and sloughed mucosa.
(Right) Axial CECT in the same case shows a generalized ileus . The colon is massively distended with blood and debris and its wall is relatively thin. Soon after this scan, the colon perforated and a total colectomy was required.
TERMINOLOGY
Definitions
• Acute transmural fulminant colitis with neuromuscular degeneration and colonic dilation
IMAGING
General Features
• Best diagnostic clue
Dilated ahaustral colon with pseudopolyps and air-fluid levels
• Location
Transverse colon > other segments
Radiographic Findings
• Radiography
Hallmark: Marked colonic dilatation with abnormal or absent fold pattern
– Transverse colon most common ± other segments
– Increased colon caliber on serial radiographs
> 5 cm on CT, often > 8 cm (as measured on supine radiograph)
– Transverse colonic folds may be thickened (edema or hemorrhage), or lost (sloughed mucosa and submucosa)
– Mucosal islands or pseudopolyps cause irregular surface contour
– Pneumatosis coli ± pneumoperitoneum
CT Findings
• Colon distended with gas, fluid ± blood
• Distorted or absent transverse fold pattern
• Irregular nodular contour of colonic wall (mucosal pseudopolyps)
• ± intramural gas ± blood
• ± free intraperitoneal gas and fluid
Imaging Recommendations
• Best imaging tool
Buy Membership for Radiology Category to continue reading. Learn more here









 .
.
 , marked dilation of the colon with loss of transverse folds, and intraluminal high-density material
, marked dilation of the colon with loss of transverse folds, and intraluminal high-density material  representing hemorrhage and sloughed mucosa.
representing hemorrhage and sloughed mucosa.
 . The colon
. The colon  is massively distended with blood and debris and its wall is relatively thin. Soon after this scan, the colon perforated and a total colectomy was required.
is massively distended with blood and debris and its wall is relatively thin. Soon after this scan, the colon perforated and a total colectomy was required.


















 , suggesting mucosal sloughing or pseudopolyps.
, suggesting mucosal sloughing or pseudopolyps.
 within the dilated, thin-walled transverse colon.
within the dilated, thin-walled transverse colon.
 , distention and thinning of the walls of the colon, as well as more mucosal pseudopolyps
, distention and thinning of the walls of the colon, as well as more mucosal pseudopolyps  .
.
 . Because of symptoms that were refractory to medical management, as well as these CT findings, the patient had a total colectomy.
. Because of symptoms that were refractory to medical management, as well as these CT findings, the patient had a total colectomy.
 in a case of toxic megacolon.
in a case of toxic megacolon.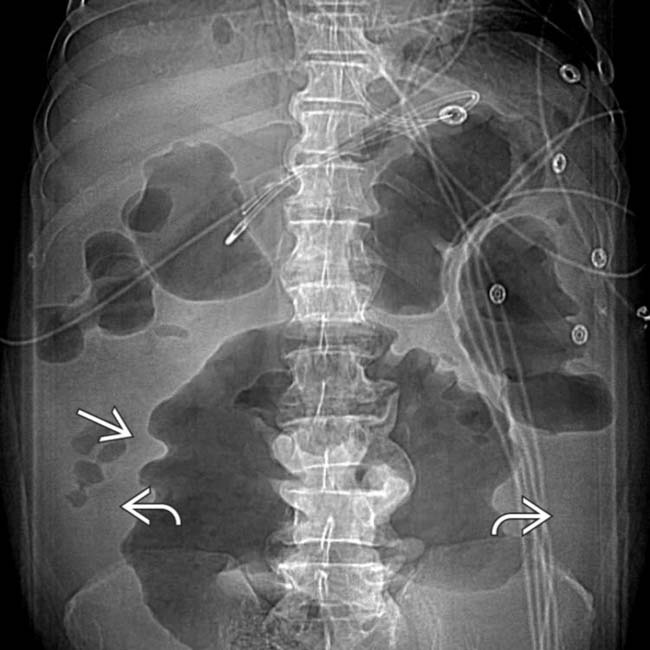
 due to ascites. The colon is diffusely dilated with a loss of the normal transverse fold pattern. The folds that are seen are grossly thickened and have a “thumbprint” appearance
due to ascites. The colon is diffusely dilated with a loss of the normal transverse fold pattern. The folds that are seen are grossly thickened and have a “thumbprint” appearance  .
.
 and colonic distension
and colonic distension  .
.
 . No normal transverse folds are evident. Ascites fills the paracolic gutters
. No normal transverse folds are evident. Ascites fills the paracolic gutters  , accounting for the bulging flanks seen on plain films.
, accounting for the bulging flanks seen on plain films.
 .
.
 with a complete loss of its normal transverse fold pattern.
with a complete loss of its normal transverse fold pattern.
 and ascites
and ascites  . These CT and clinical features are classic for toxic megacolon due to infectious colitis (C. difficile), confirmed at urgent colectomy. The colonic mucosa showed extensive necrosis and sloughing, but no frank perforation was found.
. These CT and clinical features are classic for toxic megacolon due to infectious colitis (C. difficile), confirmed at urgent colectomy. The colonic mucosa showed extensive necrosis and sloughing, but no frank perforation was found.
 due to subserosal and omental edema.
due to subserosal and omental edema.
 .
.
 .
.
 indicating edematous mucosa.
indicating edematous mucosa.

