CECT: Mural thickening of duodenum ± adjacent inflammation
TOP DIFFERENTIAL DIAGNOSES
• Cholecystitis
• Pancreatitis
• Ureteral colic
PATHOLOGY
• Gastritis commonly coexists with duodenitis
Similar findings of mucosal erosions, fold thickening, luminal spasm
CLINICAL ISSUES
• Most common signs/symptoms
Abdominal pain, nausea, vomiting
• Other signs/symptoms
Gastrointestinal bleeding with deeper ulceration
• Epidemiology
Helicobacter pylori infection and NSAID use
• Treated with proton-pump inhibitors (plus antibiotics for H. pylori)
DIAGNOSTIC CHECKLIST
• Duodenitis often coexists with gastritis
• Symptoms are indistinguishable from peptic ulcers
Presence of only superficial (aphthous) erosions and fold thickening distinguishes duodenitis from duodenal ulcer
• Diagnosis usually established by endoscopy
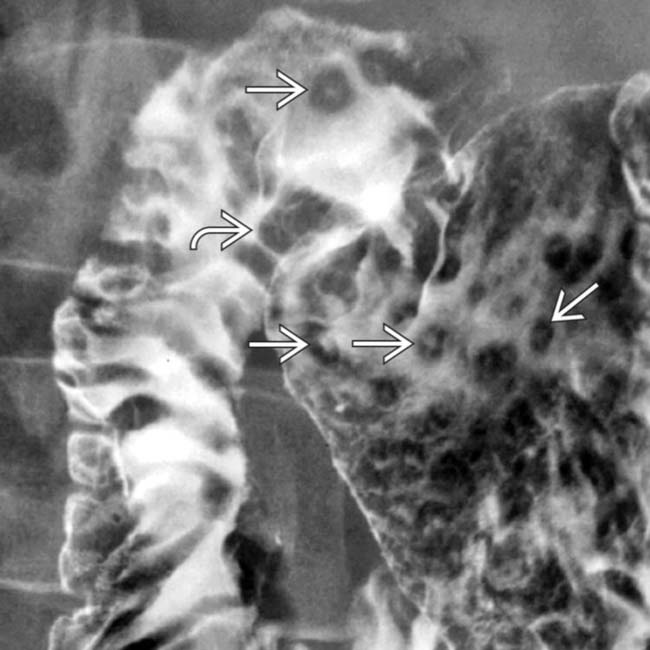
(Left) Spot film from an upper GI series shows aphthous ulcers in the gastric antrum and duodenal bulb, along with thickened duodenal folds , classic features of duodenitis and gastritis.
(Right) Spot film from an upper GI series shows nodular fold thickening and lack of distensibility in the gastric antrum due to gastritis.
(Left) Another spot film from the upper GI series shows spasm and fold thickening of the duodenum , due to duodenitis.
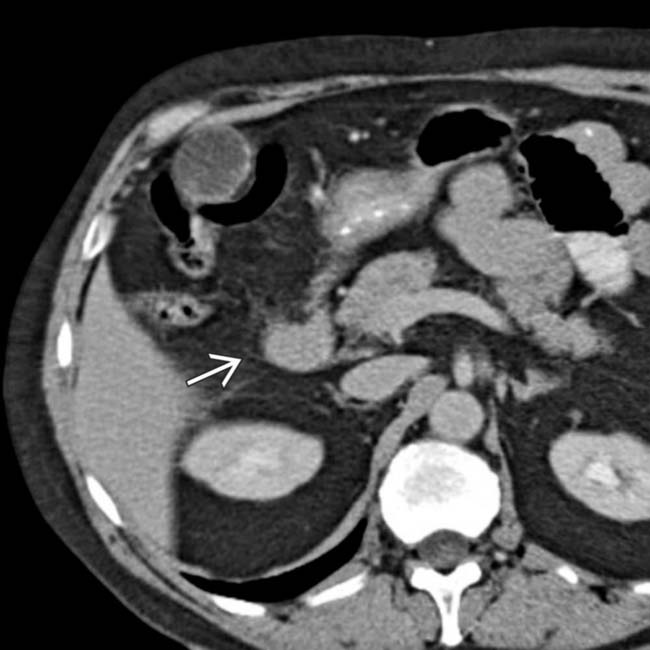
(Right) Axial CECT in the same patient shows luminal narrowing and mural thickening of the 2nd portion of duodenum, with surrounding inflammation due to duodenitis.
TERMINOLOGY
Definitions
• Duodenal inflammation from any cause
IMAGING
General Features
• Best diagnostic clue
Upper GI: Aphthous ulcers in duodenal bulb; fold thickening in antrum and duodenal bulb
CECT: Mural thickening of duodenum ± adjacent inflammation
• Location
Duodenum
• Size
Ulcers 3-7 mm
• Morphology
Discrete erosions with surrounding mound of edema in ring-like fashion
Imaging Recommendations
• Best imaging tool
Upper GI, CECT
• Protocol advice
Oral and IV contrast
Radiographic Findings
• Radiography
Ectopic gas in retroperitoneal space, free air, gastric distension
Fluoroscopic Findings
• Upper GI
Duodenal spasm, fold thickening
Superficial or deep ulcerations
Delayed gastric emptying or outlet obstruction
CT Findings
• CECT
Duodenal narrowing, fold thickening, gastric distension with air or fluid
Ectopic gas or fluid with perforation
Extravasation of oral contrast into anterior pararenal space or peritoneal cavity
Fluid adjacent to thickened duodenum
Ultrasonographic Findings
• Mural thickening of duodenum
• Fluid in anterior pararenal space
DIFFERENTIAL DIAGNOSIS
Cholecystitis
• Gallstones on US or CT, stone impacted in gallbladder neck, mural thickening > 3 mm
• Positive sonographic Murphy sign
• Pericholecystic fat stranding in omentum on CECT
Pancreatitis
• Diffuse or focal pancreatic enlargement
• Peripancreatic fluid or infiltration
Especially along Gerota fascia, anterior pararenal spaces, lesser sac, transverse mesocolon
• Nonenhancing areas on CECT if necrosis present
Ureteral Colic
• Nephromegaly, hydronephrosis, high-attenuation stone in ureter
• Perirenal fluid due to forniceal rupture
Annular Pancreas
• Congenital anomaly due to persistence of 2 ventral buds of pancreas
• Uncinate tissue surrounds duodenum, potentially mimicking mural thickening from inflammation or tumor
• May cause gastric outlet obstruction
• Presents in 1st decade; 1/2 of patients present in adulthood
Duodenal Trauma
• Duodenum may be crushed against vertebral body in rapid deceleration injuries
• Pediatric patients often develop duodenal hematoma without perforation
Best treated conservatively if no extravasation on UGI
• Perforation results in ectopic gas and fluid in anterior pararenal space
PATHOLOGY
General Features
• Etiology
Helicobacter pylori infection is most common etiology
Nonsteroidal anti-inflammatory drug (NSAID) use is next most common cause
Much less common causes
– Crohn disease
– Radiation therapy
– Pancreatitis
– Viral or other bacterial infection
– Sarcoidosis
• Associated abnormalities
Gastritis commonly coexists with duodenitis
– Similar findings of mucosal erosions, fold thickening, luminal spasm
Staging, Grading, & Classification
• Duodenitis ± perforation
Gross Pathologic & Surgical Features
• Inflammation of mucosa and submucosal edema
• Superficial (aphthous) erosions or deep ulcers
Microscopic Features
• Mucosal ulceration
• Submucosal inflammatory infiltrate
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
Abdominal pain, nausea, vomiting
• Other signs/symptoms
Gastrointestinal bleeding with deeper ulceration
Demographics
• Age
Usually > 40 years old
Children can be affected, especially with causes other than H. pylori infection
• Epidemiology
H. pylori infection
Increases with age
– 20% occurrence rate at age 20, 40% occurrence rate at age 40, 60% occurrence rate at age 60
Natural History & Prognosis
• Can cause chronic pain, perforation, and GI bleeding
• Rarely strictures result from inadequate treatment
May cause symptoms of gastric outlet obstruction
Treatment
• H. pylori treated with antibiotics and proton-pump inhibitors (PPIs)
Usually 2 antibiotics and protein pump inhibitor
• Peptic ulcer disease treated with PPIs alone
DIAGNOSTIC CHECKLIST
Consider
• Duodenitis often coexists with gastritis
• Symptoms are indistinguishable from peptic ulcers
Diagnosis usually established by endoscopy
Image Interpretation Pearls
• Presence of only superficial (aphthous) erosions and fold thickening distinguishes duodenitis from duodenal ulcer
Upper GI series in the same patient illustrates a spasm of the same portion of the duodenum, as well as duodenal fold thickening .
Axial CECT in a 64-year-old man who presented with upper abdominal pain, nausea, and vomiting demonstrates luminal narrowing and mural thickening of the 2nd portion of the duodenum, with surrounding inflammation .
CECT: Mural thickening of duodenum ± adjacent inflammation
TOP DIFFERENTIAL DIAGNOSES
• Cholecystitis
• Pancreatitis
• Ureteral colic
PATHOLOGY
• Gastritis commonly coexists with duodenitis
Similar findings of mucosal erosions, fold thickening, luminal spasm
CLINICAL ISSUES
• Most common signs/symptoms
Abdominal pain, nausea, vomiting
• Other signs/symptoms
Gastrointestinal bleeding with deeper ulceration
• Epidemiology
Helicobacter pylori infection and NSAID use
• Treated with proton-pump inhibitors (plus antibiotics for H. pylori)
DIAGNOSTIC CHECKLIST
• Duodenitis often coexists with gastritis
• Symptoms are indistinguishable from peptic ulcers
Presence of only superficial (aphthous) erosions and fold thickening distinguishes duodenitis from duodenal ulcer
• Diagnosis usually established by endoscopy
(Left) Spot film from an upper GI series shows aphthous ulcers in the gastric antrum and duodenal bulb, along with thickened duodenal folds , classic features of duodenitis and gastritis.
(Right) Spot film from an upper GI series shows nodular fold thickening and lack of distensibility in the gastric antrum due to gastritis.
(Left) Another spot film from the upper GI series shows spasm and fold thickening of the duodenum , due to duodenitis.
(Right) Axial CECT in the same patient shows luminal narrowing and mural thickening of the 2nd portion of duodenum, with surrounding inflammation due to duodenitis.
TERMINOLOGY
Definitions
• Duodenal inflammation from any cause
IMAGING
General Features
• Best diagnostic clue
Upper GI: Aphthous ulcers in duodenal bulb; fold thickening in antrum and duodenal bulb
CECT: Mural thickening of duodenum ± adjacent inflammation
• Location
Duodenum
• Size
Ulcers 3-7 mm
• Morphology
Discrete erosions with surrounding mound of edema in ring-like fashion
Imaging Recommendations
• Best imaging tool
Upper GI, CECT
• Protocol advice
Oral and IV contrast
Radiographic Findings
• Radiography
Buy Membership for Radiology Category to continue reading. Learn more here







 in the gastric antrum and duodenal bulb, along with thickened duodenal folds
in the gastric antrum and duodenal bulb, along with thickened duodenal folds  , classic features of duodenitis and gastritis.
, classic features of duodenitis and gastritis.
 and lack of distensibility in the gastric antrum due to gastritis.
and lack of distensibility in the gastric antrum due to gastritis.
 , due to duodenitis.
, due to duodenitis.
 due to duodenitis.
due to duodenitis.






























 .
.
 .
.