[level-membership-for-radiology-category] Reformat in sagittal plane to see aorta and SMA
• Antiperistaltic flow of barium proximal to obstruction
• Relief of obstruction in prone, knee-chest, or left lateral decubitus positions
TOP DIFFERENTIAL DIAGNOSES
• Duodenal obstruction (other causes)
• Intestinal scleroderma
• Duodenal stricture
PATHOLOGY
• Predisposing conditions
Weight loss → depletion of retroperitoneal fat, leading to narrowed aorto-mesenteric angle
Anatomical and congenital anomalies
Postoperative states (e.g., scoliosis)
CLINICAL ISSUES
• Postprandial epigastric pain, nausea, vomiting
Pain relieved in prone, knee-chest, or left lateral decubitus position
• Surgery (bypassing duodenum) indicated when conservative therapy fails
DIAGNOSTIC CHECKLIST
• Can be mimicked by or made worse by other causes of duodenal dilation (e.g., scleroderma)
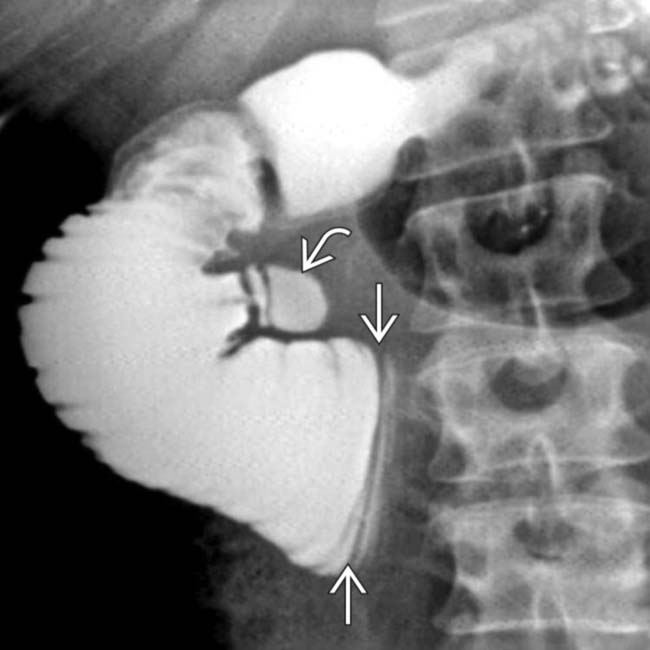
(Left) Supine film from an upper GI series in a woman with recent weight loss and early satiety shows an abrupt, straight-line cut-off of the 3rd portion of duodenum as it crosses over the midline, with dilation and slow emptying of the proximal duodenum. There is also a duodenal diverticulum .
(Right) Axial CECT shows marked distention of the 2nd portion of the duodenum and stomach. The 3rd portion of the duodenum is compressed as it passes between the aorta and the superior mesenteric artery (SMA).
(Left) Coronal reformatted CT in the same case shows dilation of the second portion of duodenum , while the remaining bowel is collapsed. Note this patient’s thin body habitus.
(Right) Sagittal-reformatted CT in the same case shows a very narrow angle between the superior mesenteric artery and the aorta, with compression of the 3rd portion of duodenum as it passes between these vessels.
TERMINOLOGY
Definitions
• Vascular compression of 3rd portion of duodenum between aorta and superior mesenteric artery (SMA)
IMAGING
General Features
• Best diagnostic clue
Dilated 1st and 2nd portions of duodenum with abrupt, straight-line transition to collapsed duodenum as it crosses spine
Imaging Recommendations
• Best imaging tool
Barium upper GI series with CECT
• Protocol advice
Obtain thin slice CECT with good contrast bolus
– Reformat in sagittal plane to see aorta and SMA
Fluoroscopic Findings
• Dilatation of 1st and 2nd portions of duodenum ± gastric dilatation
• Antiperistaltic flow of barium proximal to obstruction
• Relief of obstruction in prone, knee-chest, or left lateral decubitus positions
CT Findings
• CECT
Beak-like compression of 3rd part of duodenum between SMA and aorta
Aorto-SMA angle < 22-25° in sagittal plane
Aorto-SMA distance < 8 mm
DIFFERENTIAL DIAGNOSIS
Duodenal Obstruction (Other Causes)
• Gastroduodenoscopy is needed to rule out intraluminal causes
• Other causes of duodenal obstruction (e.g., cancer) can mimic or exacerbate SMA syndrome
Intestinal Scleroderma
• Dilated atonic small bowel with crowded folds and wide-mouthed sacculations
• Check for other small bowel, lung, or skin changes of scleroderma
Duodenal Stricture
• Usually postinflammatory with prior history of ulcer disease
• More common in proximal duodenum
PATHOLOGY
General Features
• Etiology
Impingement of 3rd duodenum by aorta and SMA
• Predisposing conditions
Weight loss → depletion of retroperitoneal fat leads to narrowed aorto-mesenteric angle
– Chronic wasting diseases
Cancer, paraplegia, cardiac cachexia, drug abuse, body casts
– Anorexia nervosa, malabsorption
– Catabolic states
Burn, trauma
Anatomical/congenital anomalies
– High insertion of ligament of Treitz → cephalad dislocation of duodenum
– Intestinal malrotation
– Low origin of SMA → decreased aorto-mesenteric distance
– Lumbar lordosis
Postoperative states
– Scoliosis surgery
– Bariatric surgery
– Nissen fundoplication
– Aortic aneurysm repair
– Ileoanal pouch anastomosis → mesenteric tension → caudal pull of SMA → ↓ aorto-mesenteric angle
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
Postprandial epigastric pain, nausea, vomiting
Pain relieved in prone, knee-chest, or left lateral decubitus position
• Other signs/symptoms
Anorexia, weight loss
Demographics
• Gender
More common in women
Natural History & Prognosis
• Good response to medical and surgical treatments
Treatment
• Acute symptoms
NG tube decompression of stomach
• Medical treatment
Increase body weight by tube feeding or parenteral nutrition
• Surgery
Indicated when conservative therapy fails
Gastrojejunostomy, duodenojejunostomy
DIAGNOSTIC CHECKLIST
Consider
• Can be mimicked by or made worse by other causes of duodenal dilation
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Reformat in sagittal plane to see aorta and SMA
• Antiperistaltic flow of barium proximal to obstruction
• Relief of obstruction in prone, knee-chest, or left lateral decubitus positions
TOP DIFFERENTIAL DIAGNOSES
• Duodenal obstruction (other causes)
• Intestinal scleroderma
• Duodenal stricture
PATHOLOGY
• Predisposing conditions
Weight loss → depletion of retroperitoneal fat, leading to narrowed aorto-mesenteric angle
Anatomical and congenital anomalies
Postoperative states (e.g., scoliosis)
CLINICAL ISSUES
• Postprandial epigastric pain, nausea, vomiting
Pain relieved in prone, knee-chest, or left lateral decubitus position
• Surgery (bypassing duodenum) indicated when conservative therapy fails
DIAGNOSTIC CHECKLIST
• Can be mimicked by or made worse by other causes of duodenal dilation (e.g., scleroderma)
(Left) Supine film from an upper GI series in a woman with recent weight loss and early satiety shows an abrupt, straight-line cut-off of the 3rd portion of duodenum as it crosses over the midline, with dilation and slow emptying of the proximal duodenum. There is also a duodenal diverticulum .
(Right) Axial CECT shows marked distention of the 2nd portion of the duodenum and stomach. The 3rd portion of the duodenum is compressed as it passes between the aorta and the superior mesenteric artery (SMA).
(Left) Coronal reformatted CT in the same case shows dilation of the second portion of duodenum , while the remaining bowel is collapsed. Note this patient’s thin body habitus.
(Right) Sagittal-reformatted CT in the same case shows a very narrow angle between the superior mesenteric artery and the aorta, with compression of the 3rd portion of duodenum as it passes between these vessels.
TERMINOLOGY
Definitions
• Vascular compression of 3rd portion of duodenum between aorta and superior mesenteric artery (SMA)
IMAGING
General Features
• Best diagnostic clue
Buy Membership for Radiology Category to continue reading. Learn more here




 of the 3rd portion of duodenum as it crosses over the midline, with dilation and slow emptying of the proximal duodenum. There is also a duodenal diverticulum
of the 3rd portion of duodenum as it crosses over the midline, with dilation and slow emptying of the proximal duodenum. There is also a duodenal diverticulum  .
.
 and stomach. The 3rd portion of the duodenum
and stomach. The 3rd portion of the duodenum  is compressed as it passes between the aorta and the superior mesenteric artery (SMA).
is compressed as it passes between the aorta and the superior mesenteric artery (SMA).
 , while the remaining bowel is collapsed. Note this patient’s thin body habitus.
, while the remaining bowel is collapsed. Note this patient’s thin body habitus.
 and the aorta, with compression of the 3rd portion of duodenum
and the aorta, with compression of the 3rd portion of duodenum  as it passes between these vessels.
as it passes between these vessels.




















