[level-membership-for-radiology-category] Hernia most commonly contains loop of Ileum, although can rarely involve other pelvic viscera (i.e., bladder)
Most often trapped between obturator externus and pectineus muscles
May also be located between superior and middle fasciculi of obturator externus or between internal and external obturator muscles
• Hernia sac exits pelvis near obturator vessels and nerve
• Right side more common
TOP DIFFERENTIAL DIAGNOSES
• Inguinal hernia
• Sciatic hernia
• Perineal hernia
• Femoral hernia
PATHOLOGY
• Defect in pelvic floor or laxity of pelvic muscles and fascia
• Made worse by any chronic increase in abdominal pressure (COPD, constipation, pregnancy, etc.)
• More common in thin or emaciated patients, as preperitoneal fat usually supports obturator canal
CLINICAL ISSUES
• Accounts for < 1% of all hernias
• > 90% occur in elderly women (mean age 82)
Less common complication of pelvic floor laxity
• Acute or recurrent small bowel obstruction, partial > complete
80% of patients present with symptoms of bowel obstruction
Majority require resection of strangulated small bowel
• Rare occurrence and nonspecific signs often lead to late diagnosis
Correct clinical diagnosis in only 10–30% of cases
Diagnosis best made by CT/MR rather than clinical exam
(Left) Graphic shows a bowel obstruction caused by an obturator hernia. Strangulated bowel lies deep to the pectineus muscle and superficial to the obturator externus muscle .
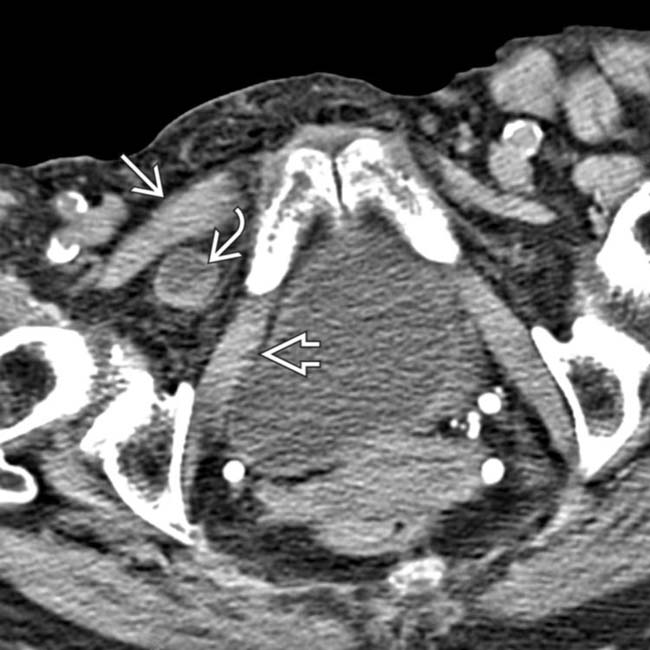
(Right) Axial CECT in a 73-year-old woman shows a protrusion of portions of the bladder into bilateral obturator hernias . Obturator hernias most commonly contain herniated ileum, but other pelvic viscera can also herniate, as in this case.
(Left) Axial CECT in a 90-year-old woman with bowel obstruction shows dilated proximal small bowel loops and collapsed distal bowel .
(Right) Axial CECT in the same patient shows the herniated and strangulated segment of the ileum trapped between the obturator externus and the pectineus muscles. These are the classic imaging findings of an obturator hernia.
TERMINOLOGY
Abbreviations
• Obturator hernia (OH)
Definitions
• Pelvic hernia protruding through obturator foramen
IMAGING
General Features
• Best diagnostic clue
CT evidence of herniated bowel lying between pectineus and obturator muscles in an elderly woman
Radiographic Findings
• Abdominal radiographs or barium studies
Small bowel obstruction with a fixed loop containing gas or contrast medium in obturator region
CT Findings
• Loop of bowel protruding through obturator foramen
Hernia most commonly contains loop of Ileum, although can rarely involve other pelvic viscera (i.e., bladder)
Most often trapped between obturator externus and pectineus muscles
• 3 forms of hernia (in decreasing frequency)
Extending between pectineus and obturator muscles
Between superior and middle fasciculi of obturator externus
Between internal and external obturator muscles
• Hernia sac exits pelvis near obturator vessels and nerve
• Right side is more common
Imaging Recommendations
• Best imaging tool
CECT: Images should include inferior pelvis and upper thigh to ensure hernia is fully imaged
DIFFERENTIAL DIAGNOSIS
Inguinal Hernia
• Abdominal contents within inguinal canal with extension into scrotum
• Does not involve obturator foramen
• Indirect: Through inguinal canal → external ring
Females: Course of round ligament into labium majus
Males: Along spermatic cord → scrotum
Sciatic Hernia
• Hernia extends through greater sciatic foramen with extension laterally into subgluteal region
Perineal Hernia
• Anterior: Through urogenital diaphragm
• Posterior: Between levator ani and coccygeus muscle
Femoral Hernia
• Hernia extends through femoral ring into femoral canal medial to femoral vein
PATHOLOGY
General Features
• Etiology
Defect in pelvic floor or laxity of pelvic muscles and fascia
Made worse by any chronic increase in abdominal pressure (COPD, constipation, pregnancy, etc.)
More common in thin or emaciated patients, as preperitoneal fat usually supports obturator canal
• Associated abnormalities
May be coexistent with other hernias (e.g., inguinal, femoral)
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
Acute or recurrent small bowel obstruction, partial > complete
– 80% of patients present with symptoms of bowel obstruction
– Obstruction is more likely to be intermittent if Richter herniation of bowel into obturator canal
May present as tender mass in obturator region on rectal or vaginal examination
• Other signs/symptoms
Howship-Romberg sign: Pain in medial aspect of thigh/hip with abduction, extension, or internal rotation of knee; flexion relieves pain (25-50% of cases)
– Compression and irritation by hernia of the obturator nerve
Hannington-Kiff sign: Absent adductor reflex in thigh (15-50% of patients)
Obturator neuralgia: Pain or paresthesias along inner surface of thigh to knee
• Rare occurrence and nonspecific signs often lead to late diagnosis, with correct clinical diagnosis in only 10–30% of cases
Demographics
• Gender
> 90% of obturator hernias occur in elderly women (mean age 82)
– Less common complication of pelvic floor laxity (incontinence, prolapse, etc.)
• Epidemiology
Accounts for < 1% of all hernias
– Bilateral obturator hernias rare: 6% of cases
Natural History & Prognosis
• Mortality rates up to 25%
Diagnosis is elusive; best made by CT or MR rather than by clinical exam
Treatment
• Majority require resection of strangulated small bowel
• Abdominal/inguinal approach for reduction and repair
• Contralateral side exploration is recommended
DIAGNOSTIC CHECKLIST
Consider
• Obturator hernia in any elderly, debilitated, chronically ill woman with symptoms of recurrent small bowel obstruction and pain along ipsilateral thigh and knee
Axial CECT shows a knuckle of bowel lying between the pectineus and obturator muscles in a patient with a obturator hernia.
Axial CECT shows an obturator hernia with the small bowel strangulated between pectineus and obturator externus muscles.
Axial CECT shows bilateral obturator hernias . Bilateral obturator hernias are rare, accounting for only 6% of all cases.
CT shows dilated proximal and collapsed distal small bowel, indicating obstruction. The point of obstruction is a segment of small bowel entrapped within an obturator hernia.
A post-evacuation film from a contrast enema in the same patient reveals a “knuckle” of bowel within the hernia. Only 1 wall of the bowel appears to be trapped.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Hernia most commonly contains loop of Ileum, although can rarely involve other pelvic viscera (i.e., bladder)
Most often trapped between obturator externus and pectineus muscles
May also be located between superior and middle fasciculi of obturator externus or between internal and external obturator muscles
• Hernia sac exits pelvis near obturator vessels and nerve
• Right side more common
TOP DIFFERENTIAL DIAGNOSES
• Inguinal hernia
• Sciatic hernia
• Perineal hernia
• Femoral hernia
PATHOLOGY
• Defect in pelvic floor or laxity of pelvic muscles and fascia
• Made worse by any chronic increase in abdominal pressure (COPD, constipation, pregnancy, etc.)
• More common in thin or emaciated patients, as preperitoneal fat usually supports obturator canal
CLINICAL ISSUES
• Accounts for < 1% of all hernias
• > 90% occur in elderly women (mean age 82)
Less common complication of pelvic floor laxity
• Acute or recurrent small bowel obstruction, partial > complete
80% of patients present with symptoms of bowel obstruction
Majority require resection of strangulated small bowel
• Rare occurrence and nonspecific signs often lead to late diagnosis
Correct clinical diagnosis in only 10–30% of cases
Diagnosis best made by CT/MR rather than clinical exam
(Left) Graphic shows a bowel obstruction caused by an obturator hernia. Strangulated bowel lies deep to the pectineus muscle and superficial to the obturator externus muscle .
(Right) Axial CECT in a 73-year-old woman shows a protrusion of portions of the bladder into bilateral obturator hernias . Obturator hernias most commonly contain herniated ileum, but other pelvic viscera can also herniate, as in this case.
(Left) Axial CECT in a 90-year-old woman with bowel obstruction shows dilated proximal small bowel loops and collapsed distal bowel .
(Right) Axial CECT in the same patient shows the herniated and strangulated segment of the ileum trapped between the obturator externus and the pectineus muscles. These are the classic imaging findings of an obturator hernia.
TERMINOLOGY
Abbreviations
• Obturator hernia (OH)
Definitions
• Pelvic hernia protruding through obturator foramen
IMAGING
General Features
• Best diagnostic clue
CT evidence of herniated bowel lying between pectineus and obturator muscles in an elderly woman
Radiographic Findings
•
Buy Membership for Radiology Category to continue reading. Learn more here

 May also be located between superior and middle fasciculi of obturator externus or between internal and external obturator muscles
May also be located between superior and middle fasciculi of obturator externus or between internal and external obturator muscles




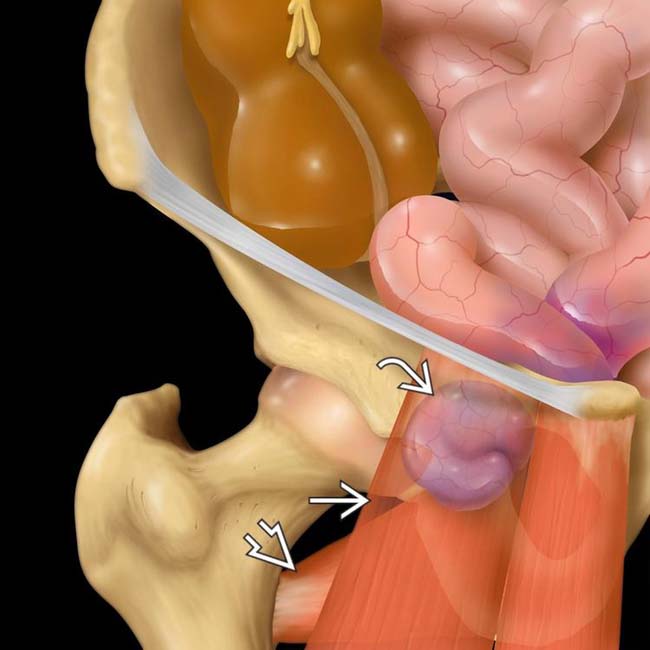
 lies deep to the pectineus muscle
lies deep to the pectineus muscle  and superficial to the obturator externus muscle
and superficial to the obturator externus muscle  .
.
 . Obturator hernias most commonly contain herniated ileum, but other pelvic viscera can also herniate, as in this case.
. Obturator hernias most commonly contain herniated ileum, but other pelvic viscera can also herniate, as in this case.
 and collapsed distal bowel
and collapsed distal bowel  .
.
 trapped between the obturator externus
trapped between the obturator externus  and the pectineus
and the pectineus  muscles. These are the classic imaging findings of an obturator hernia.
muscles. These are the classic imaging findings of an obturator hernia.





















 lying between the pectineus
lying between the pectineus  and obturator muscles
and obturator muscles  in a patient with a obturator hernia.
in a patient with a obturator hernia.
 between pectineus and obturator externus muscles.
between pectineus and obturator externus muscles.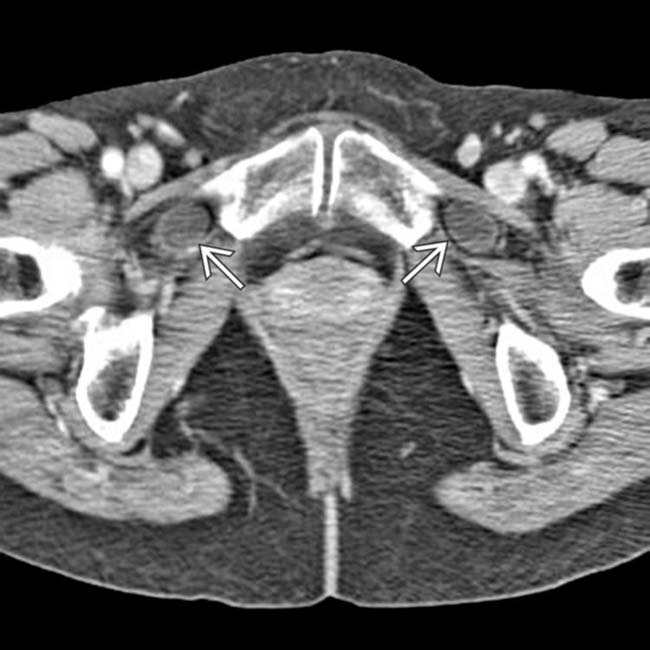
 . Bilateral obturator hernias are rare, accounting for only 6% of all cases.
. Bilateral obturator hernias are rare, accounting for only 6% of all cases.
 entrapped within an obturator hernia.
entrapped within an obturator hernia.
 within the hernia. Only 1 wall of the bowel appears to be trapped.
within the hernia. Only 1 wall of the bowel appears to be trapped.