• MR shows some elements better than CT (lipid and hemorrhage)
• Gadoxetate-enhanced MR (Eovist; Primovist)
Adenoma shows no substantial uptake or retention
Key distinction from FNH
• T1WI: Mass: Heterogeneous signal intensity
Increased signal intensity (due to fat or recent hemorrhage)
Decreased signal intensity (necrosis, calcification, old hemorrhage)
• Heterogeneous, hypervascular mass with foci of fat or hemorrhage in a young woman
TOP DIFFERENTIAL DIAGNOSES
• Hepatocellular carcinoma (HCC)
HCC typically occurs in older, cirrhotic men
• Fibrolamellar HCC
• Focal nodular hyperplasia
Homogeneously enhances; retains gadoxetate
• Hypervascular metastases
PATHOLOGY
• Hepatic steatosis, pregnancy, anabolic steroids, and oral contraceptives increase number and growth rate of adenomas
CLINICAL ISSUES
• Risk factors for HCC
Large adenoma, male sex, glycogen storage disease, anabolic steroid use, CTNNB1 -mutated subtype of HA
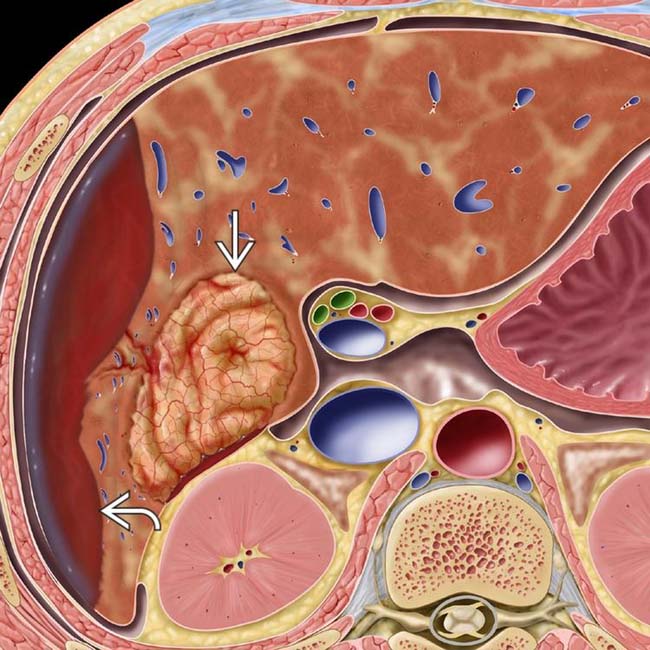
(Left) Graphic shows a hypervascular mass in the right lobe and spontaneous subcapsular bleeding .
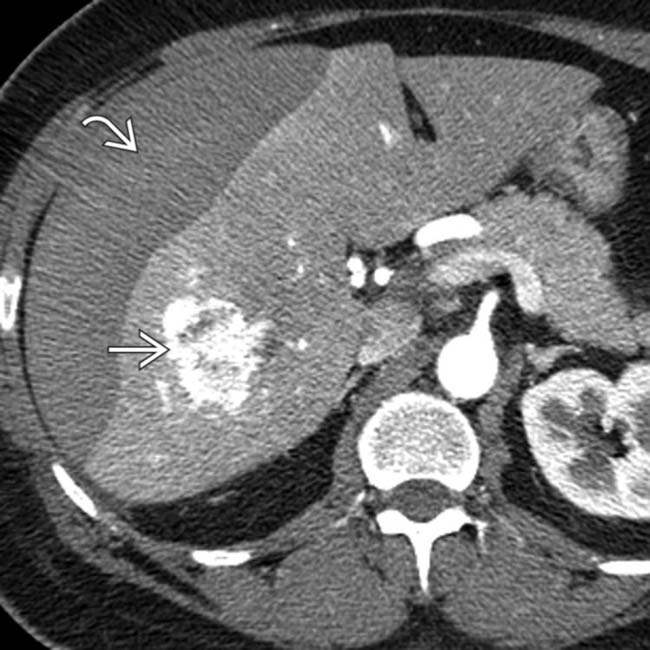
(Right) Axial CECT of a 40-year-old woman with sudden RUQ pain and syncope shows an intensely enhancing mass in the right lobe of the liver. A lentiform heterogeneous collection of fluid indents the surface of the liver, and within this collection is a focus of higher density likely representing a sentinel clot. A ruptured inflammatory hepatic adenoma was resected.
(Left) Photograph of a resected specimen shows a large adenoma with central areas of rupture and hemorrhage . (Courtesy M. Yeh, MD, PhD.)
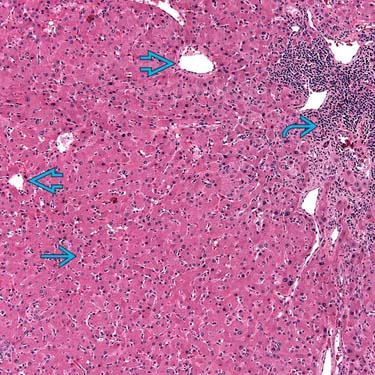
(Right) Photomicrograph of a hepatic adenoma features a thin-walled unpaired vessel surrounded by neoplastic hepatocytes with abundant steatosis. Imaging often reveals these features, directly or indirectly. (Courtesy M. Yeh, MD, PhD.)
TERMINOLOGY
Abbreviations
• Hepatic adenoma (HA)
Synonyms
• Hepatocellular adenoma, liver cell adenoma
Definitions
• Heterogeneous group of benign hepatocellular neoplasms with distinctive genetic, pathologic, and clinical features
IMAGING
General Features
• Best diagnostic clue
Heterogeneous, hypervascular mass with foci of fat or hemorrhage in a young woman
• Location
Subcapsular region of right lobe of liver (75%)
Intraparenchymal or pedunculated (10%)
• Size
Varies from 6-30 cm
• Key concepts
Very uncommon relative to focal nodular hyperplasia (FNH) and hepatocellular carcinoma (HCC)
3 distinct subtypes with different genetics, pathology, clinical features
CT Findings
• Depending on HA subtype
Encapsulation seen in ∼ 20%, best on delayed phase CECT
Hemorrhage within tumor, best seen on NECT as hyperdense foci
Intratumoral lipid, best seen on NECT as hypodense foci
Hypervascularity
– Most intense and persistent in inflammatory subtype of HA
Calcification: Focal, present in ∼ 5%
MR Findings
• T1WI
Mass: Heterogeneous signal intensity
– Increased signal intensity (due to fat and recent hemorrhage), more evident on MR than CT
– Decreased signal intensity (necrosis, calcification, old hemorrhage)
Rim (fibrous pseudocapsule): Hypointense
• T2WI
Mass: Heterogeneous signal intensity
– Increased signal intensity (old hemorrhage, necrosis)
– Decreased signal intensity (fat, recent hemorrhage)
Rim (fibrous pseudocapsule): Hypointense
• T1WI C+
Gadolinium, arterial phase
– Heterogeneous hypervascular enhancement (especially in inflammatory subtype)
Delayed phase
– Pseudocapsule: Hyperintense to liver and adenoma
• Gadoxetate-enhanced MR (Eovist, Primovist)
Hepatocellular-specific contrast agent
Adenoma shows no substantial uptake or retention on delayed imaging
– Key distinction from FNH
Ultrasonographic Findings
• Grayscale ultrasound
Complex, hyper-/hypoechoic, heterogeneous mass with anechoic areas
– Due to fat, hemorrhage, necrosis, and calcification
– Capsule may be seen
• Color Doppler
Hypervascular tumor
Large peripheral arteries and veins
Intratumoral veins present
– Absent in FNH; useful distinction for adenoma
Angiographic Findings
• Conventional
Hypervascular mass with centripetal flow
Enlarged hepatic artery with feeders at tumor periphery (50%)
Hypovascular; avascular regions
– Due to hemorrhage and necrosis
Nuclear Medicine Findings
• Technetium sulfur colloid (TcSC)
Usually “cold” (photopenic) (80%)
Uncommonly “warm” (20%)
– Due to uptake in sparse Kupffer cells
• HIDA scan
Increased activity in some
• Gallium scan
No uptake
Imaging Recommendations
• Best imaging tool
Gadoxetate-enhanced MR, including multiphasic and delayed imaging
In- and opposed-phase GRE
DIFFERENTIAL DIAGNOSIS
Hepatocellular Carcinoma
• May be hard to distinguish on imaging or pathology
• Biliary, vascular, nodal invasion and metastases = malignancy
• HCC typically occurs in older, cirrhotic men
Adenoma occurs in young, healthy women
Fibrolamellar HCC
• Large, lobulated mass with scar and septa
• Vascular, biliary invasion and metastases common
Focal Nodular Hyperplasia
• Arterial phase: Homogeneously enhancing mass
• All other phases: Isodense to normal liver
• T2WI: Scar is typically hyperintense
• Uniformly retains gadoxetate on delayed phase MR
Hypervascular Metastases
• Usually multiple; look for primary tumors
Breast, thyroid, kidney, and endocrine
• Arterial phase: Heterogeneous enhancement
• Portal and delayed phases: Iso-/hypodense washout
PATHOLOGY
General Features
• Etiology
↑ risk in oral contraceptive and anabolic steroid users
Pregnancy increases growth rate and risk of rupture
Hepatic steatosis ↑ growth and number of adenomas
Diabetes mellitus
von Gierke type I glycogen storage disease
– Multiple adenomas in 60% of affected patients
Staging, Grading, & Classification
• Proposed new classification based on genetics, pathology, and tumor biology
• 3 distinct subtypes
Inflammatory HA
– Most common subtype (40-50%)
– Includes those previously called “telangiectatic HA”
– Occur in young women on oral contraceptives and obese women
– 60% have mutation of IL6ST gene with altered glycoprotein metabolism
– MR: No excessive fat or lipid within masses; persistent hypervascularity through arterial and venous phases due to sinusoidal dilation, peliotic areas, and abnormal vessels
Bright on T2WI
Likely to show MR (and clinical) evidence of hemorrhage (up to 30%)
10% estimated likelihood of malignant degeneration to HCC
HNF1A -mutated HA
– 2nd most common subtype (30-35% of HAs)
– Association with diabetes and familial hepatic adenomatosis
– Exclusively in women; 90% have history of oral contraceptive use
– Mutated HNF1A gene promotes lipogenesis and hepatocellular proliferation
– MR: Diffuse lipid deposition within HAs
Most evident as signal dropout on opposed-phase GRE T1WI
Macroscopic fat deposits are less common
Only moderate enhancement on arterial phase; no persistent enhancement on venous and delayed
– Least aggressive subtype
HAs of this subtype < 5 cm rarely bleed and have minimal risk of HCC
CTNNB1 -mutated HA
– Least common subtype (10-15% of HAs)
– Subtype most likely to occur in men, those taking androgenic steroids, and in patients with glycogen storage disease
Also associated with metabolic syndrome
– Mutation of CTNNB1 disrupts hepatocyte proliferation, growth, adhesion, etc.
– This subtype carries highest risk of malignant transformation (> 10%)
– MR features: No distinctive pattern established
Usually hypervascular with evidence of hemorrhage or necrosis within tumor
Unclassified HA subtype
– Does not fit other profiles of HA subtypes
Gross Pathologic & Surgical Features
• Well-circumscribed mass within noncirrhotic liver
Soft, pale, or yellowish tan
Frequently bile-stained nodules
Foci of fat, hemorrhage, infarction
Pseudocapsule and occasional pseudopods
• Adenomatosis
No strict definition (generally > 10 adenomas)
Associated with glycogen storage disease, steatosis, and diabetes
May number > 100 adenomas
– May cause hepatic dysfunction, hemorrhage
Microscopic Features
• Sheets or cords of hepatocytes
• Absence of portal and central veins and bile ducts
– Not seen in males unless on anabolic steroids or with glycogen storage disease
Natural History & Prognosis
• Complications
Hemorrhage: Intrahepatic or intraperitoneal (40%)
Rupture: Increased risk in pregnancy
May regress on withdrawal of oral contraceptives
• Risk factors for degeneration into HCC
Male gender (10x more frequent than in women on per case basis)
Concomitant glycogen storage disease
Anabolic steroid use
CTNNB1 -mutated subtype of HA
HA mass size > 5 cm
• Prognosis
Usually good
– After discontinuation of oral contraceptives
– After surgical resection of large or symptomatic HAs
Poor
– Intraperitoneal rupture
– Rupture during pregnancy
– Malignant transformation
– Adenomatosis (> 10 adenomas)
May hemorrhage, impair hepatic function
Treatment
• Adenoma < 5 cm
Observation and discontinuation of oral contraceptives or other steroids
• Adenoma > 5 cm and near surface
Surgical resection
Consider transcatheter embolization
• Pregnancy should be avoided due to ↑ risk of rupture
• Transplantation for some cases of adenomatosis
DIAGNOSTIC CHECKLIST
Consider
• Rule out other benign and malignant liver tumors, which have similar imaging features
Particularly HCC or FNH
• Check for history of oral contraceptives and glycogen storage disease (in case of multiple adenomas)
Image Interpretation Pearls
• Spherical, well-defined, hypervascular, and heterogeneous mass due to hemorrhage and fat; most evident on MR
• Gadoxetate-enhanced MR is most specific imaging test
(Left) Venous phase CECT of an 18-year-old girl injured in a vehicle crash shows a subcapsular, encapsulated mass that is not very vascular, a typical (but not diagnostic) feature of the HNF1A-mutated subtype of hepatic adenoma.
(Right) An axial fat-suppressed T2WI in the same patient shows the mass as almost isointense to background liver with a thin hyperintense capsule , typical features of an HNF1A-mutated subtype of hepatic adenoma.
(Left) T1-weighted in-phase MR in the same case shows a uniform iso- to slightly hyperintense peripheral liver lesion with a thin low-intensity capsule .
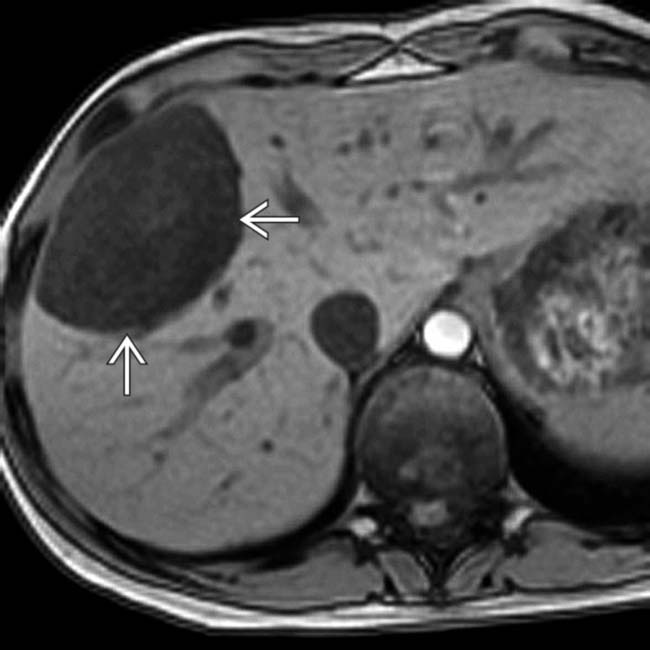
(Right) An opposed-phase GRE T1WI in the same case shows marked signal loss from the mass , which indicates the presence of diffuse lipid, another typical feature of this subtype of hepatic adenoma.
(Left) On this delayed phase image in the same case, obtained after IV administration of gadoxetate (Eovist, Primovist), the normal liver enhances brightly whereas the mass shows no retained contrast, which indicates that it lacks functioning bile ductules and differentiates it from a focal nodular hyperplasia (FNH).
(Right) Photograph of the resected specimen, an HNF1A-mutated subtype of hepatic adenoma, shows an encapsulated, pale, tan mass with diffuse and focal lipid .
(Left) Axial T1WI GRE in-phase MR in a 54-year-old woman who had a liver mass detected on CT shows the mass as slightly hyperintense to a normal-appearing liver. On opposed-phase GRE MR (not shown), there was no signal dropout from the lesion, indicating no lipid content.
(Right) On T2WI MR in the same case, the mass is slightly hyperintense to the liver, and a central scar is quite hyperintense.
(Left) On MR sections in the same case taken after bolus injection of gadoxetate (Eovist) the mass is hypervascular whereas the central scar is hypointense . The mass and central scar were nearly isointense on the venous phase images (not shown).
(Right) On a 20-minute delayed image in the same case the mass retains less contrast material than normal liver. Because there was concern that the lesion was not a typical FNH, it was resected.
(Left) Photo of the gross pathology specimen shows an encapsulated mass with blood pooling and foci of hemorrhage.
(Right) Histologic specimen in the same case shows disorganized hepatocytes with abundant eosinophilic nuclei on H&E staining, unpaired blood vessels distributed haphazardly throughout the lesion, and foci of chronic inflammation . The final diagnosis was hepatic adenoma of the inflammatory subtype. (Courtesy T. Longacre, MD.)
(Left) Axial T1WI of a 35-year-old woman with RUQ pain shows a hepatic mass containing several hyperintense foci that represent hemorrhage.
(Right) Axial T1WI shows more hyperintense foci of hemorrhage within the hypointense mass .
(Left) Axial T2WI in the same case shows a heterogeneous mass with some foci of slight hyperintensity that represent lipid.
(Right) Axial portal venous phase T1WI in the same case shows persistent hypervascular enhancement in the nonnecrotic and nonhemorrhagic portions of the mass, typical features of the inflammatory subtype of hepatic adenoma, which was confirmed on resection.
(Left) Axial NECT shows a very large, sharply demarcated, mostly homogeneous mass with a small focus of hemorrhage .
(Right) Axial arterial phase CECT in the same patient shows hypervascularity with enlarged vessels within and on the surface of the tumor. Note the large hepatic artery . Hepatic adenomas of the inflammatory subtype are usually heterogeneously hypervascular and often encapsulated with focal hemorrhage, as in this patient.
(Left) Axial opposed-phase GRE T1WI MR shows an encapsulated mass with hyperintense foci representing hemorrhage or fat. The in-phase images showed increased signal within the mass.
(Right) Axial fat-suppressed T2WI MR in the same patient shows that the mass is nearly isointense to the liver with a central focus of hyperintensity (hemorrhage). Fat content would have shown signal dropout on this sequence. A capsule or pseudocapsule is seen in ∼ 20% of adenomas.
(Left) Axial CT during the arterial phase of enhancement shows a brightly enhancing mass with a focal calcification , the latter being a less common feature of adenomas.
(Right) Ultrasound in the same case confirms the solid mass with calcification and shows a capsule around the mass. The capsule is a common feature and the focal calcification a less common feature of adenomas, as was proven in this case.
(Left) Arterial phase T1WI contrast-enhanced MR of a 32-year-old woman who had been using oral contraceptives for 14 years shows 1 of about 10 encapsulated, enhancing focal masses .
(Right) More adenomas are seen on this section. In the absence of chronic liver disease or a known malignancy, these findings were considered diagnostic of adenomas. Following cessation of oral contraceptive use, these adenomas decreased in size and number within 4 months.
(Left) Axial NECT of a 37-year-old man with type I glycogen storage disease and multiple adenomas shows hepatomegaly and low-attenuation masses within the liver. The low attenuation is due to intratumoral lipid. These are foci of the CTNNB1-mutated subtype of hepatic adenoma.
(Right) A hepatic arterial phase image in the same patient shows that some lesions are hypervascular whereas others show heterogeneous enhancement .
(Left) Portal venous phase image in the same case shows capsular enhancement or compressed hepatic parenchyma around most of the adenomas . Adenomas are usually multiple in the setting of type I or III glycogen storage disease and carry a high risk of malignant degeneration, especially those > 5 cm in diameter and those in men.
(Right) Photograph of the resected specimens in a case of hepatic adenomatosis shows multiple adenomas with hemorrhage and necrosis. (Courtesy M. Yeh, MD, PhD.)
(Left) Axial CECT shows a large heterogeneous hepatic mass with several foci measuring less than water attenuation, indicating fat content. Also noted are foci of calcification . Serial CT scans had shown slow growth of the mass over 7 years.
(Right) Gross pathology from the same case shows the mass with foci of fat and hemorrhage . Histology revealed foci of HCC within this adenoma, which had the CTNNB1 mutation, as did the foci of HCC.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Almost all in young women with high estrogen environment, including steatosis and oral contraceptive use
Anabolic steroids, diabetes, and glycogen storage disease are other causes
• MR shows some elements better than CT (lipid and hemorrhage)
• Gadoxetate-enhanced MR (Eovist; Primovist)
Adenoma shows no substantial uptake or retention
Key distinction from FNH
• T1WI: Mass: Heterogeneous signal intensity
Increased signal intensity (due to fat or recent hemorrhage)
Decreased signal intensity (necrosis, calcification, old hemorrhage)
• Heterogeneous, hypervascular mass with foci of fat or hemorrhage in a young woman
TOP DIFFERENTIAL DIAGNOSES
• Hepatocellular carcinoma (HCC)
HCC typically occurs in older, cirrhotic men
• Fibrolamellar HCC
• Focal nodular hyperplasia
Homogeneously enhances; retains gadoxetate
• Hypervascular metastases
PATHOLOGY
• Hepatic steatosis, pregnancy, anabolic steroids, and oral contraceptives increase number and growth rate of adenomas
CLINICAL ISSUES
• Risk factors for HCC
Large adenoma, male sex, glycogen storage disease, anabolic steroid use, CTNNB1 -mutated subtype of HA
(Left) Graphic shows a hypervascular mass in the right lobe and spontaneous subcapsular bleeding .
(Right) Axial CECT of a 40-year-old woman with sudden RUQ pain and syncope shows an intensely enhancing mass in the right lobe of the liver. A lentiform heterogeneous collection of fluid indents the surface of the liver, and within this collection is a focus of higher density likely representing a sentinel clot. A ruptured inflammatory hepatic adenoma was resected.
(Left) Photograph of a resected specimen shows a large adenoma with central areas of rupture and hemorrhage . (Courtesy M. Yeh, MD, PhD.)
(Right) Photomicrograph of a hepatic adenoma features a thin-walled unpaired vessel surrounded by neoplastic hepatocytes with abundant steatosis. Imaging often reveals these features, directly or indirectly. (Courtesy M. Yeh, MD, PhD.)
TERMINOLOGY
Abbreviations
• Hepatic adenoma (HA)
Synonyms
• Hepatocellular adenoma, liver cell adenoma
Definitions
• Heterogeneous group of benign hepatocellular neoplasms with distinctive genetic, pathologic, and clinical features
IMAGING
General Features
• Best diagnostic clue
Heterogeneous, hypervascular mass with foci of fat or hemorrhage in a young woman
• Location
Subcapsular region of right lobe of liver (75%)
Intraparenchymal or pedunculated (10%)
• Size
Varies from 6-30 cm
• Key concepts
Very uncommon relative to focal nodular hyperplasia (FNH) and hepatocellular carcinoma (HCC)
3 distinct subtypes with different genetics, pathology, clinical features
CT Findings
• Depending on HA subtype
Encapsulation seen in ∼ 20%, best on delayed phase CECT
Hemorrhage within tumor, best seen on NECT as hyperdense foci
Intratumoral lipid, best seen on NECT as hypodense foci
Hypervascularity
– Most intense and persistent in inflammatory subtype of HA
Calcification: Focal, present in ∼ 5%
MR Findings
• T1WI
Mass: Heterogeneous signal intensity
– Increased signal intensity (due to fat and recent hemorrhage), more evident on MR than CT
– Decreased signal intensity (necrosis, calcification, old hemorrhage)
Rim (fibrous pseudocapsule): Hypointense
• T2WI
Mass: Heterogeneous signal intensity
– Increased signal intensity (old hemorrhage, necrosis)
– Decreased signal intensity (fat, recent hemorrhage)
Rim (fibrous pseudocapsule): Hypointense
• T1WI C+
Gadolinium, arterial phase
– Heterogeneous hypervascular enhancement (especially in inflammatory subtype)
Delayed phase
– Pseudocapsule: Hyperintense to liver and adenoma
• Gadoxetate-enhanced MR (Eovist, Primovist)
Hepatocellular-specific contrast agent
Adenoma shows no substantial uptake or retention on delayed imaging
– Key distinction from FNH
Ultrasonographic Findings
• Grayscale ultrasound
Complex, hyper-/hypoechoic, heterogeneous mass with anechoic areas
– Due to fat, hemorrhage, necrosis, and calcification
– Capsule may be seen
• Color Doppler
Hypervascular tumor
Large peripheral arteries and veins
Intratumoral veins present
– Absent in FNH; useful distinction for adenoma
Angiographic Findings
• Conventional
Hypervascular mass with centripetal flow
Enlarged hepatic artery with feeders at tumor periphery (50%)
Hypovascular; avascular regions
– Due to hemorrhage and necrosis
Nuclear Medicine Findings
• Technetium sulfur colloid (TcSC)
Usually “cold” (photopenic) (80%)
Uncommonly “warm” (20%)
– Due to uptake in sparse Kupffer cells
• HIDA scan
Increased activity in some
• Gallium scan
No uptake
Imaging Recommendations
• Best imaging tool
Gadoxetate-enhanced MR, including multiphasic and delayed imaging
In- and opposed-phase GRE
DIFFERENTIAL DIAGNOSIS
Hepatocellular Carcinoma
• May be hard to distinguish on imaging or pathology
• Biliary, vascular, nodal invasion and metastases = malignancy
• HCC typically occurs in older, cirrhotic men
Adenoma occurs in young, healthy women
Fibrolamellar HCC
• Large, lobulated mass with scar and septa
•
Buy Membership for Radiology Category to continue reading. Learn more here








 in the right lobe and spontaneous subcapsular bleeding
in the right lobe and spontaneous subcapsular bleeding  .
.
 in the right lobe of the liver. A lentiform heterogeneous collection of fluid indents the surface of the liver, and within this collection is a focus of higher density
in the right lobe of the liver. A lentiform heterogeneous collection of fluid indents the surface of the liver, and within this collection is a focus of higher density  likely representing a sentinel clot. A ruptured inflammatory hepatic adenoma was resected.
likely representing a sentinel clot. A ruptured inflammatory hepatic adenoma was resected.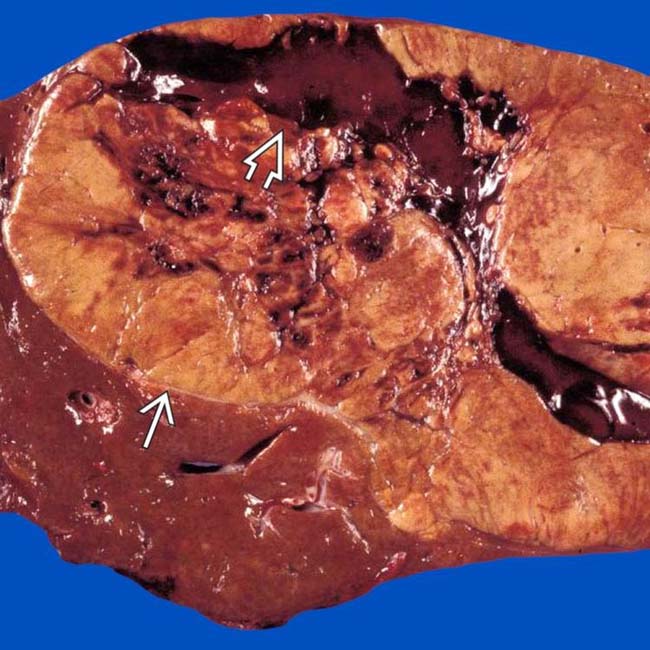
 with central areas of rupture and hemorrhage
with central areas of rupture and hemorrhage  . (Courtesy M. Yeh, MD, PhD.)
. (Courtesy M. Yeh, MD, PhD.)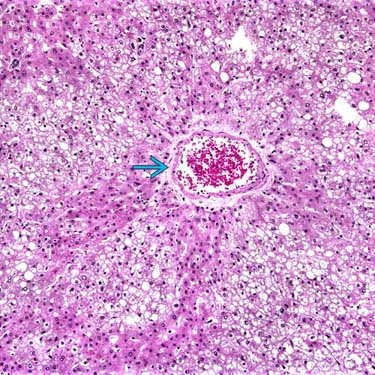
 surrounded by neoplastic hepatocytes with abundant steatosis. Imaging often reveals these features, directly or indirectly. (Courtesy M. Yeh, MD, PhD.)
surrounded by neoplastic hepatocytes with abundant steatosis. Imaging often reveals these features, directly or indirectly. (Courtesy M. Yeh, MD, PhD.)






































 Inflammatory HA
Inflammatory HA









































 that is not very vascular, a typical (but not diagnostic) feature of the HNF1A-mutated subtype of hepatic adenoma.
that is not very vascular, a typical (but not diagnostic) feature of the HNF1A-mutated subtype of hepatic adenoma.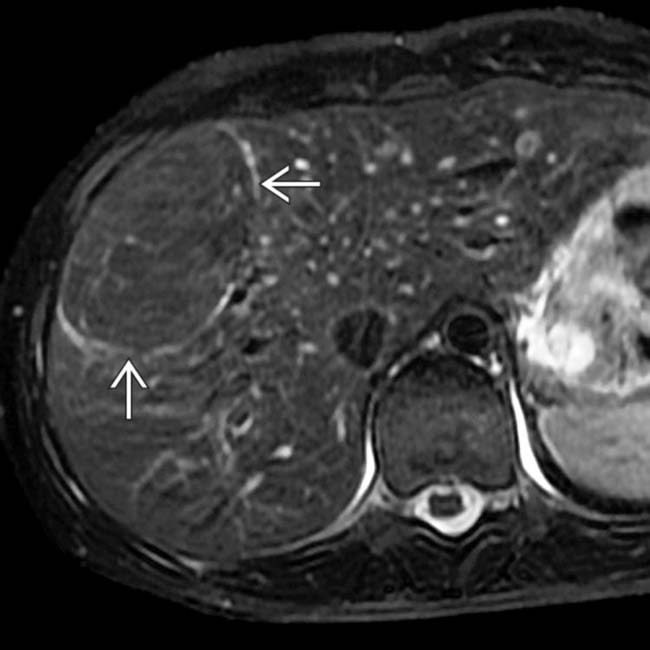
 , typical features of an HNF1A-mutated subtype of hepatic adenoma.
, typical features of an HNF1A-mutated subtype of hepatic adenoma.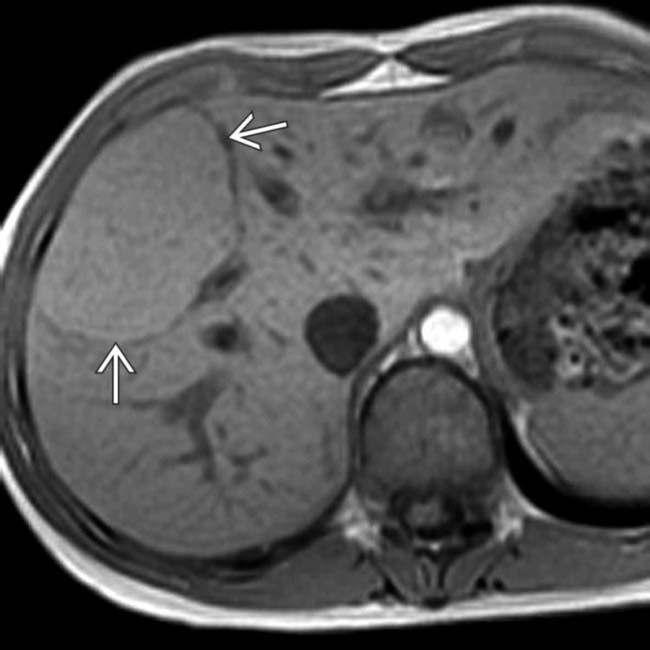
 .
.
 , which indicates the presence of diffuse lipid, another typical feature of this subtype of hepatic adenoma.
, which indicates the presence of diffuse lipid, another typical feature of this subtype of hepatic adenoma.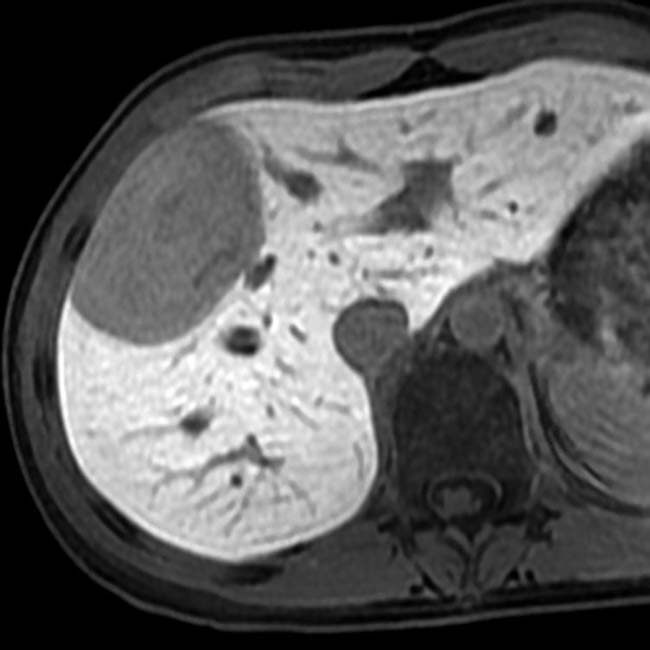
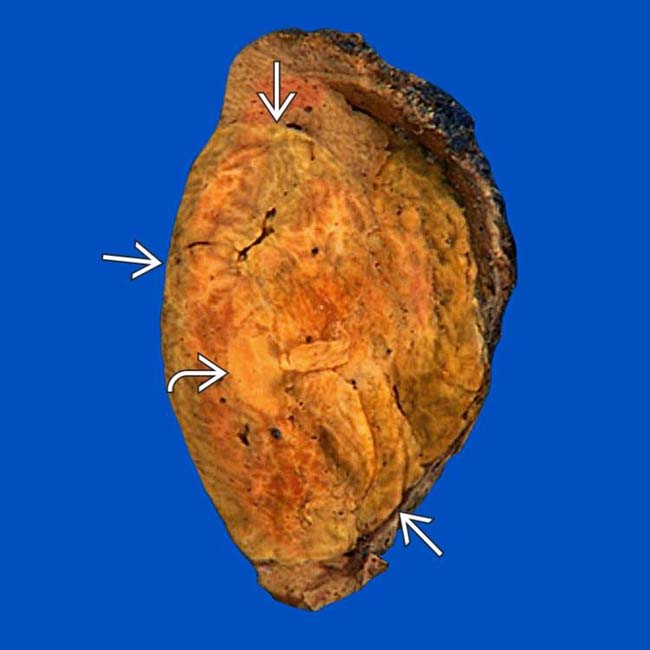
 with diffuse and focal lipid
with diffuse and focal lipid  .
.
 as slightly hyperintense to a normal-appearing liver. On opposed-phase GRE MR (not shown), there was no signal dropout from the lesion, indicating no lipid content.
as slightly hyperintense to a normal-appearing liver. On opposed-phase GRE MR (not shown), there was no signal dropout from the lesion, indicating no lipid content.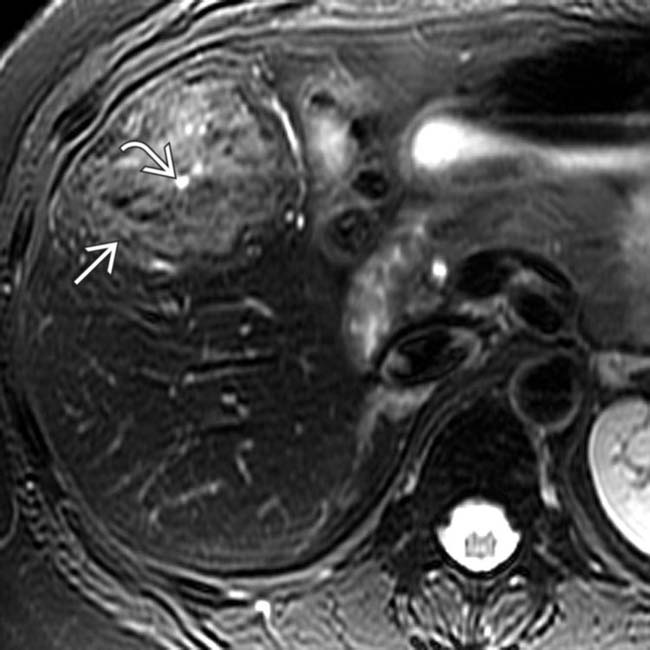
 is slightly hyperintense to the liver, and a central scar
is slightly hyperintense to the liver, and a central scar  is quite hyperintense.
is quite hyperintense.
 whereas the central scar is hypointense
whereas the central scar is hypointense  . The mass and central scar were nearly isointense on the venous phase images (not shown).
. The mass and central scar were nearly isointense on the venous phase images (not shown).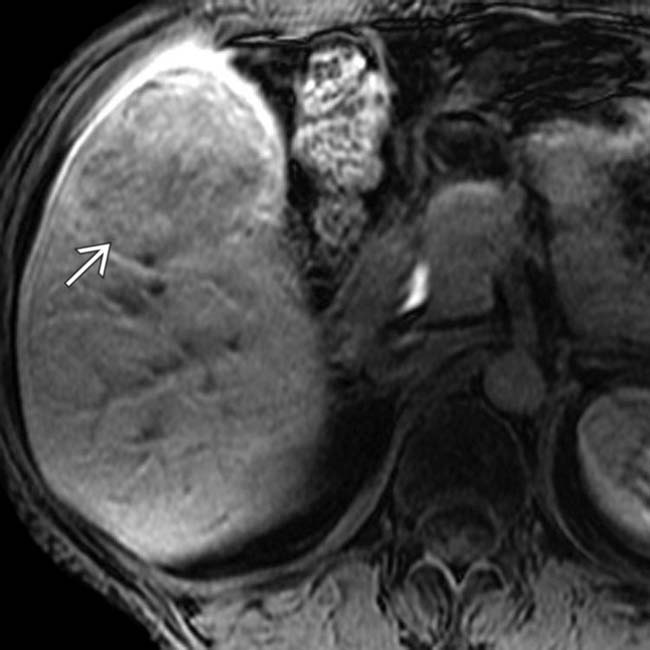
 retains less contrast material than normal liver. Because there was concern that the lesion was not a typical FNH, it was resected.
retains less contrast material than normal liver. Because there was concern that the lesion was not a typical FNH, it was resected.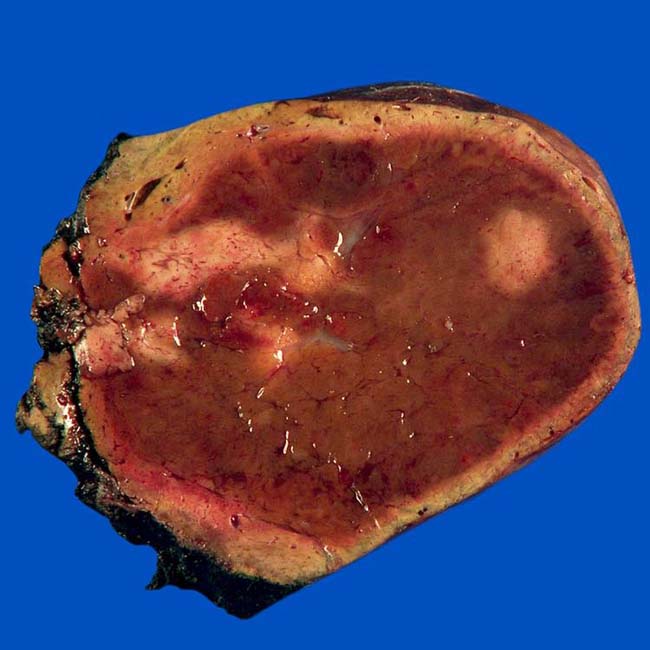
 with abundant eosinophilic nuclei on H&E staining, unpaired blood vessels
with abundant eosinophilic nuclei on H&E staining, unpaired blood vessels  distributed haphazardly throughout the lesion, and foci of chronic inflammation
distributed haphazardly throughout the lesion, and foci of chronic inflammation  . The final diagnosis was hepatic adenoma of the inflammatory subtype. (Courtesy T. Longacre, MD.)
. The final diagnosis was hepatic adenoma of the inflammatory subtype. (Courtesy T. Longacre, MD.)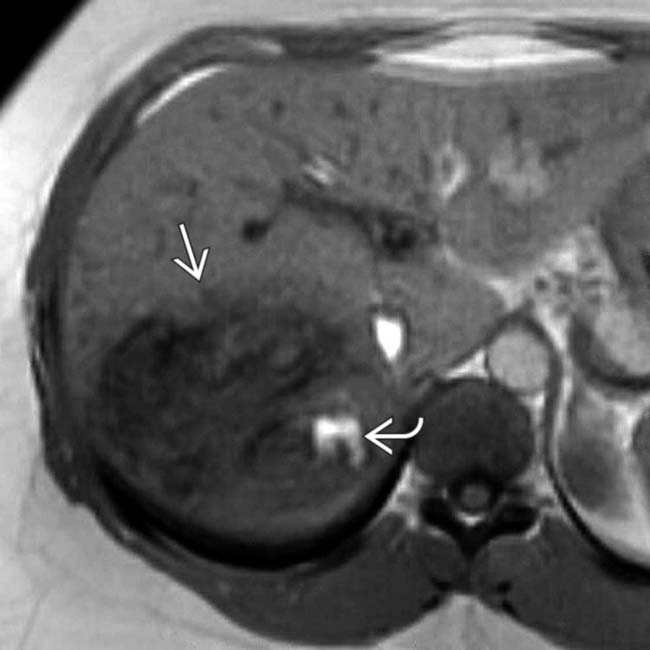
 containing several hyperintense foci
containing several hyperintense foci  that represent hemorrhage.
that represent hemorrhage.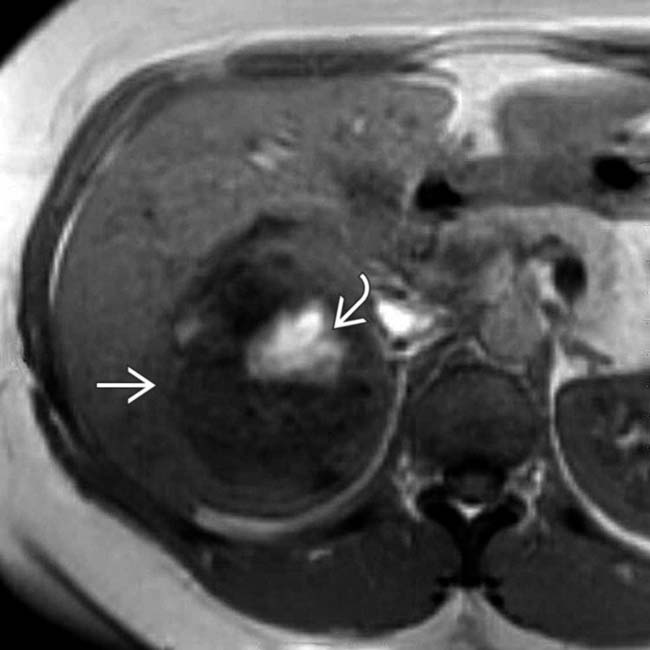
 of hemorrhage within the hypointense mass
of hemorrhage within the hypointense mass  .
.
 that represent lipid.
that represent lipid.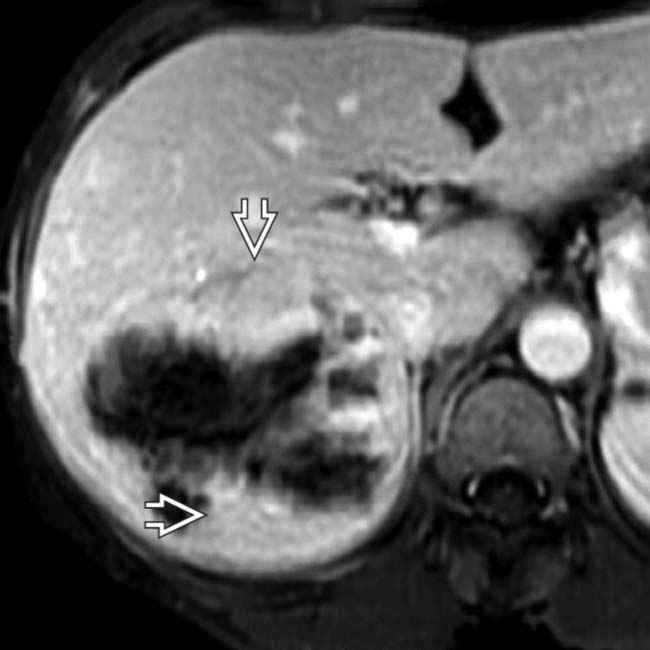
 in the nonnecrotic and nonhemorrhagic portions of the mass, typical features of the inflammatory subtype of hepatic adenoma, which was confirmed on resection.
in the nonnecrotic and nonhemorrhagic portions of the mass, typical features of the inflammatory subtype of hepatic adenoma, which was confirmed on resection.
 .
.
 . Hepatic adenomas of the inflammatory subtype are usually heterogeneously hypervascular and often encapsulated with focal hemorrhage, as in this patient.
. Hepatic adenomas of the inflammatory subtype are usually heterogeneously hypervascular and often encapsulated with focal hemorrhage, as in this patient.
 with hyperintense foci
with hyperintense foci  representing hemorrhage or fat. The in-phase images showed increased signal within the mass.
representing hemorrhage or fat. The in-phase images showed increased signal within the mass.
 (hemorrhage). Fat content would have shown signal dropout on this sequence. A capsule or pseudocapsule is seen in ∼ 20% of adenomas.
(hemorrhage). Fat content would have shown signal dropout on this sequence. A capsule or pseudocapsule is seen in ∼ 20% of adenomas.
 with a focal calcification
with a focal calcification  , the latter being a less common feature of adenomas.
, the latter being a less common feature of adenomas.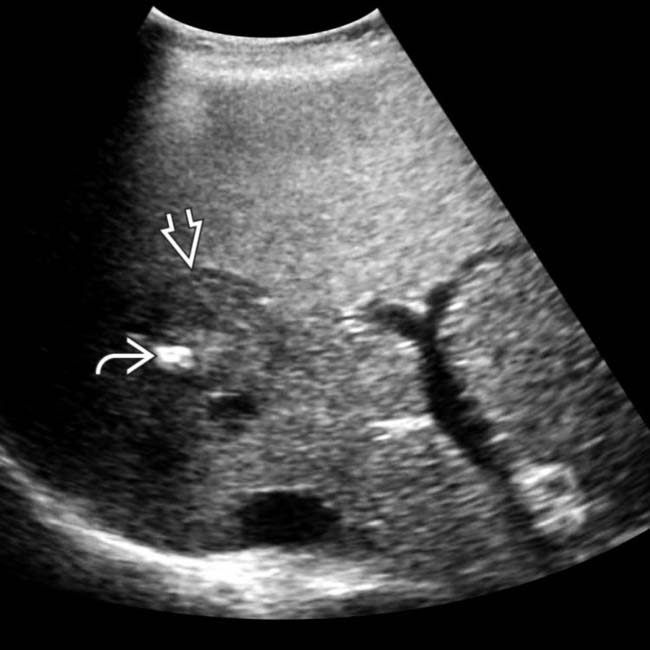
 and shows a capsule
and shows a capsule  around the mass. The capsule is a common feature and the focal calcification a less common feature of adenomas, as was proven in this case.
around the mass. The capsule is a common feature and the focal calcification a less common feature of adenomas, as was proven in this case.
 .
.
 are seen on this section. In the absence of chronic liver disease or a known malignancy, these findings were considered diagnostic of adenomas. Following cessation of oral contraceptive use, these adenomas decreased in size and number within 4 months.
are seen on this section. In the absence of chronic liver disease or a known malignancy, these findings were considered diagnostic of adenomas. Following cessation of oral contraceptive use, these adenomas decreased in size and number within 4 months.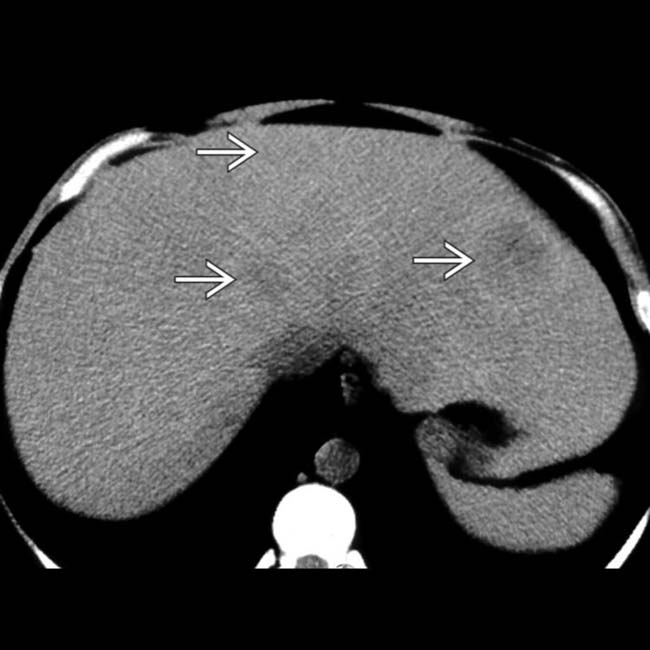
 within the liver. The low attenuation is due to intratumoral lipid. These are foci of the CTNNB1-mutated subtype of hepatic adenoma.
within the liver. The low attenuation is due to intratumoral lipid. These are foci of the CTNNB1-mutated subtype of hepatic adenoma.
 whereas others show heterogeneous enhancement
whereas others show heterogeneous enhancement  .
.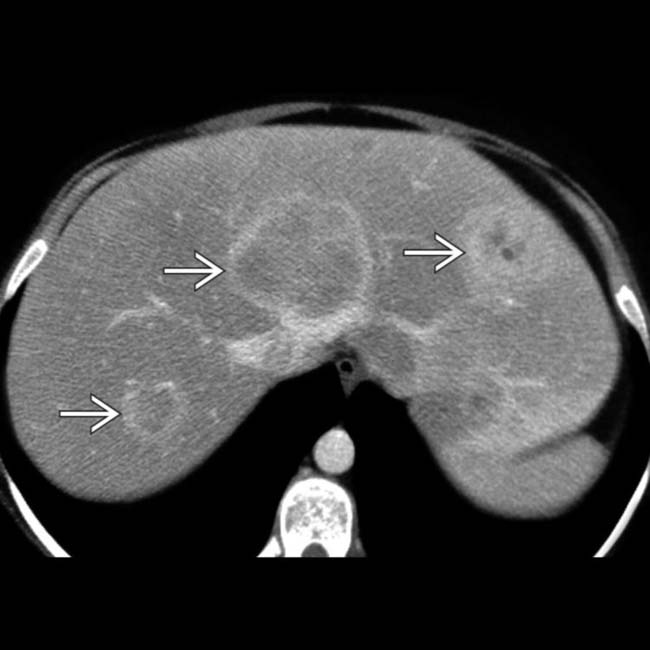
 . Adenomas are usually multiple in the setting of type I or III glycogen storage disease and carry a high risk of malignant degeneration, especially those > 5 cm in diameter and those in men.
. Adenomas are usually multiple in the setting of type I or III glycogen storage disease and carry a high risk of malignant degeneration, especially those > 5 cm in diameter and those in men.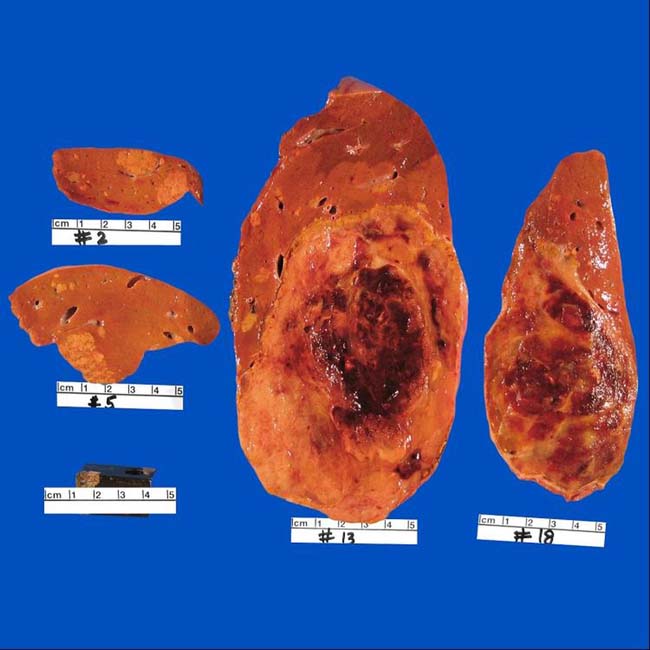

 measuring less than water attenuation, indicating fat content. Also noted are foci of calcification
measuring less than water attenuation, indicating fat content. Also noted are foci of calcification  . Serial CT scans had shown slow growth of the mass over 7 years.
. Serial CT scans had shown slow growth of the mass over 7 years.
 and hemorrhage
and hemorrhage  . Histology revealed foci of HCC within this adenoma, which had the CTNNB1 mutation, as did the foci of HCC.
. Histology revealed foci of HCC within this adenoma, which had the CTNNB1 mutation, as did the foci of HCC.