[level-membership-for-radiology-category] Pure form: Affects only pancreaticoduodenal groove
Segmental form: Affects pancreaticoduodenal groove and extends medially into pancreatic head
• Pancreatic groove is a theoretical space defined by pancreatic head (medially), 2nd portion of duodenum (laterally), 3rd portion of duodenum and IVC (posteriorly), and duodenal bulb (superiorly)
IMAGING
• Sheet-like, curvilinear soft tissue mass between pancreatic head and duodenum
May demonstrate delayed enhancement
MR: Usually T1 hypointense with variable T2 signal (depending on acuity)
• Thickened medial duodenal wall ± cysts within groove or thickened duodenal wall
• Segmental form: Mass-like enlargement of pancreatic head
• Calcifications and ductal dilatation/beading can develop in chronic setting (similar to traditional chronic pancreatitis)
TOP DIFFERENTIAL DIAGNOSES
• Pancreatic ductal adenocarcinoma
• Duodenal carcinoma
• Acute edematous pancreatitis involving groove
CLINICAL ISSUES
• Usually middle-aged men with history of alcohol abuse
• Amylase, lipase, and tumor markers are usually normal
• Prospective diagnosis is very uncommon; difficult to exclude malignancy with imaging or biopsy
• Surgery (Whipple procedure) may be required to rule out malignancy or due to intractable symptoms
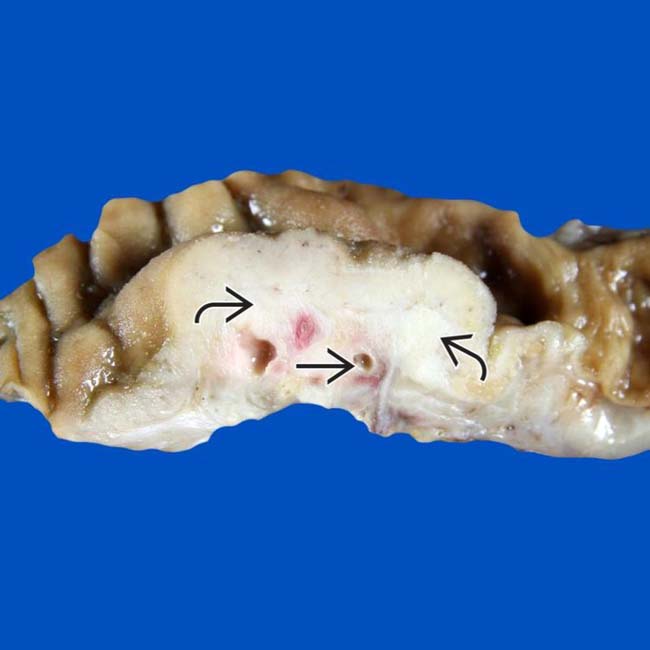
(Left) Gross photo of a pancreaticoduodenectomy specimen shows a mass-like lesion beneath the duodenal mucosa, representing groove pancreatitis. Note the paraduodenal zone of fibrosis with numerous small cysts .
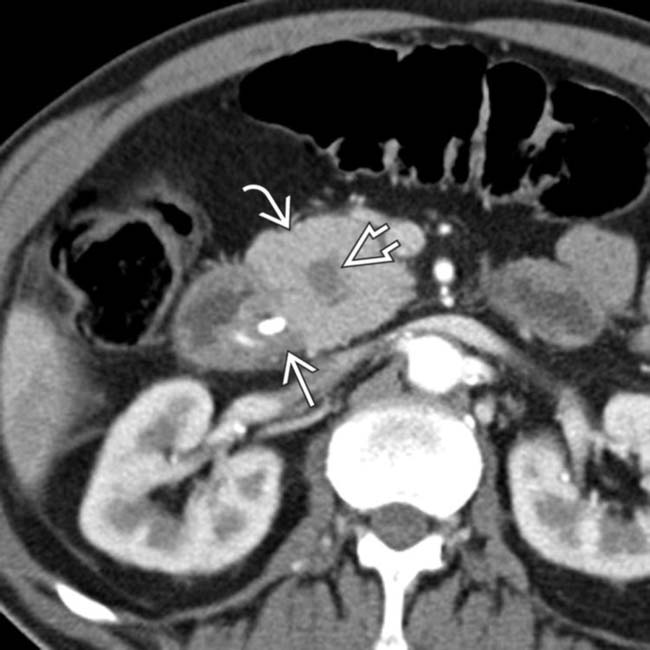
(Right) Axial CECT shows subtle soft tissue thickening in the pancreaticoduodenal groove, as well as mass-like pancreatic head enlargement with an internal cyst . This was found to be segmental (given pancreatic head involvement) groove pancreatitis at surgery.
(Left) Axial CECT image demonstrates a hypodense soft tissue mass in the pancreaticoduodenal groove with associated cystic spaces , resulting in upstream pancreatic ductal dilatation .
(Right) Coronal volume-rendered CECT image nicely demonstrates the hypodense soft tissue in the pancreaticoduodenal groove with associated cystic spaces . Initially suspected to represent malignancy, this was found to be groove pancreatitis at surgery.
TERMINOLOGY
Synonyms
• Cystic dystrophy of duodenal wall, pancreatic hamartoma of duodenal wall, periampullary duodenal wall cyst
Definitions
• Form of chronic pancreatitis affecting pancreaticoduodenal groove
Pure form: Affects only pancreaticoduodenal groove
Segmental form: Affects pancreaticoduodenal groove and extends medially into pancreatic head
• Pancreatic groove is a theoretical space defined by pancreatic head (medially), 2nd portion of duodenum (laterally), 3rd portion of duodenum and IVC (posteriorly), and duodenal bulb (superiorly)
Contains distal common bile duct (CBD), main/accessory pancreatic ducts, and major/minor papilla
IMAGING
General Features
• Best diagnostic clue
Curvilinear soft tissue between pancreas and duodenum
CT Findings
• Sheet-like, curvilinear soft tissue mass (with delayed enhancement) between pancreatic head and duodenum
• Narrowing of distal CBD and pancreatic duct at ampulla
• Absence of retroperitoneal inflammation or fluid
• Segmental form: Mass-like enlargement of pancreatic head
• Calcifications and ductal beading in chronic setting
MR Findings
• Sheet-like groove thickening is mildly T1 hypointense
• Variable T2 signal (depending on acuity): T2 hyperintense in acute phase and hypointense chronically
T2 hyperintense cysts in medial duodenal wall or groove
• Pancreatic head may be enlarged with low T1 signal in segmental form (due to fibrosis/atrophy)
• T1WI C+: Delayed enhancement of affected areas
• MRCP: Smooth narrowing of distal CBD and pancreatic duct with widened space between ampulla and duodenal lumen
Ultrasonographic Findings
• Acute setting: Hypoechoic band-like thickening in groove (with hypoechoic, heterogeneous pancreatic head in segmental form)
• Chronic setting: Hyperechoic band-like thickening in groove (with hyperechoic pancreatic head in segmental form)
Imaging Recommendations
• Best imaging tool
CECT or MR with MRCP
DIFFERENTIAL DIAGNOSIS
Pancreatic Ductal Adenocarcinoma
• Infiltrative hypodense mass with upstream pancreatic atrophy and pancreatic ductal dilatation
• May be centered in close proximity to groove and appear indistinguishable from groove pancreatitis
• Thickening of duodenal wall or cystic change is uncommon
Duodenal Carcinoma
• Mass centered in duodenum (not in pancreatic groove) without cystic change
Acute Edematous Pancreatitis Involving Groove
• Not primarily centered in pancreaticoduodenal groove and usually involves entire pancreas
• Associated with peripancreatic inflammation, including retroperitoneal fluid and fat stranding
• Should resolve on follow-up examinations
PATHOLOGY
General Features
• Etiology
Exact cause unknown, although there are multiple theories
– Alcohol consumption or smoking → increased viscosity of pancreatic juice → occlusion of minor papilla
– Functional obstruction of minor papilla/Santorini duct
– Heterotopic pancreas in duodenal wall
– Peptic ulcer disease and Brunner gland hyperplasia
Gross Pathologic & Surgical Features
• Fibrotic mass-like thickening in pancreaticoduodenal groove and stenosis of terminal CBD
• Involved areas can have internal cysts (± internal calculi)
Microscopic Features
• Thickening of duodenal wall and adjacent pancreas
• Brunner gland and smooth muscle hyperplasia
• Chronic pancreatitis ± calcification
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
Acute setting: Postprandial abdominal pain, nausea, and vomiting
Chronic setting: Chronic weight loss, jaundice
Amylase, lipase, and tumor markers usually normal
• Other signs/symptoms
Demographics
• Often middle-aged men with history of alcohol abuse
Natural History & Prognosis
• May progress to generalized chronic pancreatitis
Treatment
• Prospective diagnosis is very uncommon; difficult (or impossible) to exclude malignancy with imaging or biopsy
• Surgery (Whipple procedure) may be required to rule out malignancy or due to intractable symptoms
• Fasting, parenteral nutrition, and cessation of smoking/alcohol if prospective diagnosis is made
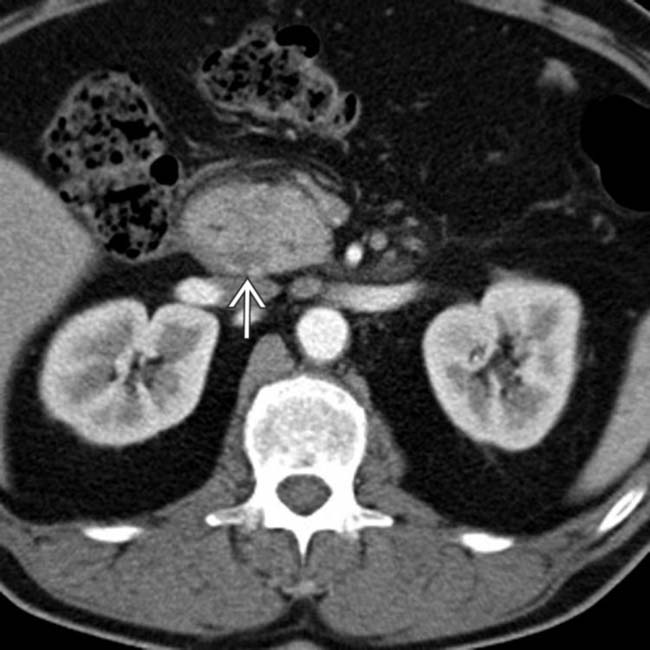
(Left) Axial CECT demonstrates subtle stranding and induration in the pancreaticoduodenal groove, which persisted on follow-up examinations.
(Right) Axial CECT image from the same patient again demonstrates induration in the pancreaticoduodenal groove. Initially suspected to represent a duodenal malignancy, this was found to be groove pancreatitis at surgery.
(Left) Axial CECT shows focal soft tissue thickening in the pancreaticoduodenal groove, which persisted over multiple follow-up studies. There is also some fluid tracking from the groove into the right anterior pararenal space.
(Right) Axial CECT in the same patient shows thickening in the groove, with several cysts present in the pancreatic head. This was found to be groove pancreatitis at surgery, but the presence of fluid tracking in the retroperitoneum is atypical and more common with acute edematous pancreatitis.
(Left) Axial CECT demonstrates focal soft tissue thickening in the pancreaticoduodenal groove with multiple internal cystic spaces .
(Right) Coronal volume-rendered CECT from the same patient again demonstrates focal soft tissue thickening in the pancreaticoduodenal groove with multiple internal cystic spaces . While this was suspected to represent groove pancreatitis, Whipple procedure was performed to exclude underlying malignancy, a common outcome in these cases.
(Left) Axial CECT shows a markedly distended stomach and proximal duodenum secondary to gastric outlet obstruction. Note the band-like soft tissue thickening in the groove between the 2nd duodenum and the pancreas, characteristic of groove pancreatitis.
(Right) More caudal CECT from the same patient shows that the lumen of the 2nd portion of duodenum is markedly narrowed by the adjacent soft tissue, and there is a small cyst in the pancreatic groove.
(Left) Axial CECT shows thickening of the medial wall of the duodenum, luminal narrowing, and 2 small cysts . This was found to represent groove pancreatitis at surgery.
(Right) Axial CECT image demonstrates a fibroinflammatory mass with calcifications centered in the groove. Groove pancreatitis in the chronic setting, as in this case, can appear very similar to traditional chronic pancreatitis (including the presence of calcifications).
(Left) Axial CECT shows low-attenuation soft tissue thickening in the groove between the head of the pancreas and the 2nd duodenum . Note the stent in the common duct placed due to biliary obstruction from the adjacent soft tissue.
(Right) Axial volume-rendered CECT shows that the hypodense soft tissue encases the gastroduodenal artery and thickens the medial wall of the 2nd duodenum .
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Pure form: Affects only pancreaticoduodenal groove
Segmental form: Affects pancreaticoduodenal groove and extends medially into pancreatic head
• Pancreatic groove is a theoretical space defined by pancreatic head (medially), 2nd portion of duodenum (laterally), 3rd portion of duodenum and IVC (posteriorly), and duodenal bulb (superiorly)
IMAGING
• Sheet-like, curvilinear soft tissue mass between pancreatic head and duodenum
May demonstrate delayed enhancement
MR: Usually T1 hypointense with variable T2 signal (depending on acuity)
• Thickened medial duodenal wall ± cysts within groove or thickened duodenal wall
• Segmental form: Mass-like enlargement of pancreatic head
• Calcifications and ductal dilatation/beading can develop in chronic setting (similar to traditional chronic pancreatitis)
TOP DIFFERENTIAL DIAGNOSES
• Pancreatic ductal adenocarcinoma
• Duodenal carcinoma
• Acute edematous pancreatitis involving groove
CLINICAL ISSUES
• Usually middle-aged men with history of alcohol abuse
• Amylase, lipase, and tumor markers are usually normal
• Prospective diagnosis is very uncommon; difficult to exclude malignancy with imaging or biopsy
• Surgery (Whipple procedure) may be required to rule out malignancy or due to intractable symptoms
(Left) Gross photo of a pancreaticoduodenectomy specimen shows a mass-like lesion beneath the duodenal mucosa, representing groove pancreatitis. Note the paraduodenal zone of fibrosis with numerous small cysts .
(Right) Axial CECT shows subtle soft tissue thickening in the pancreaticoduodenal groove, as well as mass-like pancreatic head enlargement with an internal cyst . This was found to be segmental (given pancreatic head involvement) groove pancreatitis at surgery.
(Left) Axial CECT image demonstrates a hypodense soft tissue mass in the pancreaticoduodenal groove with associated cystic spaces , resulting in upstream pancreatic ductal dilatation .
(Right) Coronal volume-rendered CECT image nicely demonstrates the hypodense soft tissue in the pancreaticoduodenal groove with associated cystic spaces . Initially suspected to represent malignancy, this was found to be groove pancreatitis at surgery.
TERMINOLOGY
Synonyms
• Cystic dystrophy of duodenal wall, pancreatic hamartoma of duodenal wall, periampullary duodenal wall cyst
Definitions
• Form of chronic pancreatitis affecting pancreaticoduodenal groove
Pure form: Affects only pancreaticoduodenal groove
Segmental form: Affects pancreaticoduodenal groove and extends medially into pancreatic head
• Pancreatic groove is a theoretical space defined by pancreatic head (medially), 2nd portion of duodenum (laterally), 3rd portion of duodenum and IVC (posteriorly), and duodenal bulb (superiorly)
Contains distal common bile duct (CBD), main/accessory pancreatic ducts, and major/minor papilla
IMAGING
General Features
• Best diagnostic clue
Curvilinear soft tissue between pancreas and duodenum
CT Findings
• Sheet-like, curvilinear soft tissue mass (with delayed enhancement) between pancreatic head and duodenum



 beneath the duodenal mucosa, representing groove pancreatitis. Note the paraduodenal zone of fibrosis with numerous small cysts
beneath the duodenal mucosa, representing groove pancreatitis. Note the paraduodenal zone of fibrosis with numerous small cysts  .
.
 in the pancreaticoduodenal groove, as well as mass-like pancreatic head
in the pancreaticoduodenal groove, as well as mass-like pancreatic head  enlargement with an internal cyst
enlargement with an internal cyst  . This was found to be segmental (given pancreatic head involvement) groove pancreatitis at surgery.
. This was found to be segmental (given pancreatic head involvement) groove pancreatitis at surgery.
 in the pancreaticoduodenal groove with associated cystic spaces
in the pancreaticoduodenal groove with associated cystic spaces  , resulting in upstream pancreatic ductal dilatation
, resulting in upstream pancreatic ductal dilatation  .
.
 in the pancreaticoduodenal groove with associated cystic spaces
in the pancreaticoduodenal groove with associated cystic spaces  . Initially suspected to represent malignancy, this was found to be groove pancreatitis at surgery.
. Initially suspected to represent malignancy, this was found to be groove pancreatitis at surgery.









 in the pancreaticoduodenal groove, which persisted on follow-up examinations.
in the pancreaticoduodenal groove, which persisted on follow-up examinations.
 in the pancreaticoduodenal groove. Initially suspected to represent a duodenal malignancy, this was found to be groove pancreatitis at surgery.
in the pancreaticoduodenal groove. Initially suspected to represent a duodenal malignancy, this was found to be groove pancreatitis at surgery.
 in the pancreaticoduodenal groove, which persisted over multiple follow-up studies. There is also some fluid
in the pancreaticoduodenal groove, which persisted over multiple follow-up studies. There is also some fluid  tracking from the groove into the right anterior pararenal space.
tracking from the groove into the right anterior pararenal space.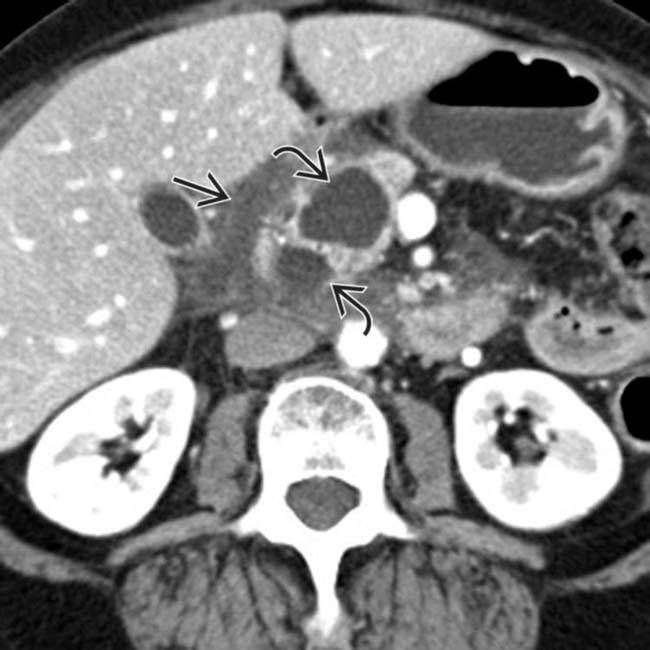
 in the groove, with several cysts
in the groove, with several cysts  present in the pancreatic head. This was found to be groove pancreatitis at surgery, but the presence of fluid tracking in the retroperitoneum is atypical and more common with acute edematous pancreatitis.
present in the pancreatic head. This was found to be groove pancreatitis at surgery, but the presence of fluid tracking in the retroperitoneum is atypical and more common with acute edematous pancreatitis.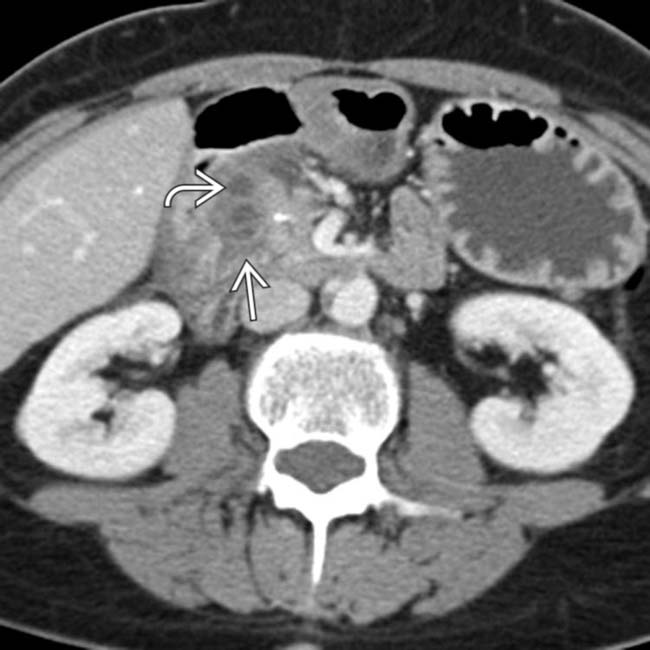
 in the pancreaticoduodenal groove with multiple internal cystic spaces
in the pancreaticoduodenal groove with multiple internal cystic spaces  .
.
 in the pancreaticoduodenal groove with multiple internal cystic spaces
in the pancreaticoduodenal groove with multiple internal cystic spaces  . While this was suspected to represent groove pancreatitis, Whipple procedure was performed to exclude underlying malignancy, a common outcome in these cases.
. While this was suspected to represent groove pancreatitis, Whipple procedure was performed to exclude underlying malignancy, a common outcome in these cases.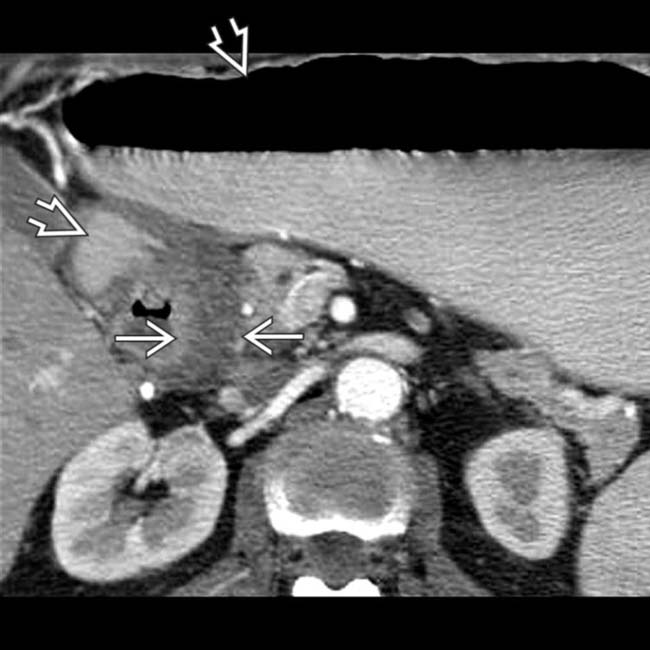
 secondary to gastric outlet obstruction. Note the band-like soft tissue thickening
secondary to gastric outlet obstruction. Note the band-like soft tissue thickening  in the groove between the 2nd duodenum and the pancreas, characteristic of groove pancreatitis.
in the groove between the 2nd duodenum and the pancreas, characteristic of groove pancreatitis.
 is markedly narrowed by the adjacent soft tissue, and there is a small cyst
is markedly narrowed by the adjacent soft tissue, and there is a small cyst  in the pancreatic groove.
in the pancreatic groove.
 . This was found to represent groove pancreatitis at surgery.
. This was found to represent groove pancreatitis at surgery.
 centered in the groove. Groove pancreatitis in the chronic setting, as in this case, can appear very similar to traditional chronic pancreatitis (including the presence of calcifications).
centered in the groove. Groove pancreatitis in the chronic setting, as in this case, can appear very similar to traditional chronic pancreatitis (including the presence of calcifications).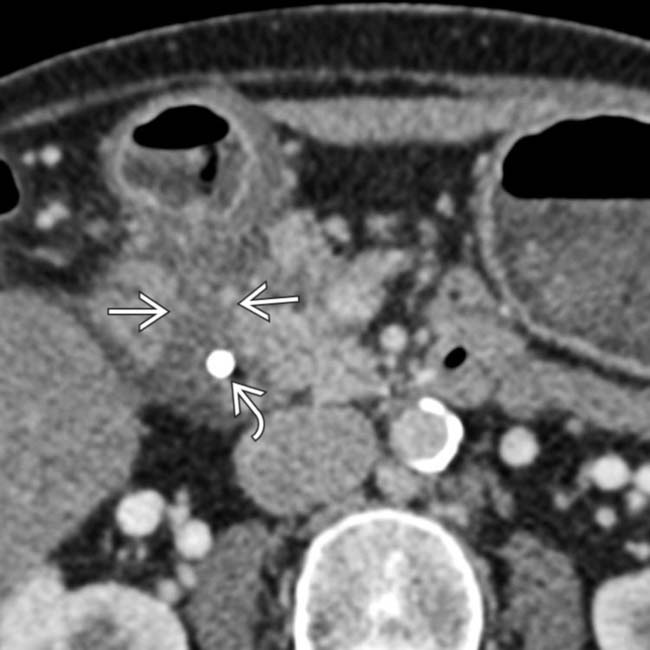
 . Note the stent
. Note the stent  in the common duct placed due to biliary obstruction from the adjacent soft tissue.
in the common duct placed due to biliary obstruction from the adjacent soft tissue.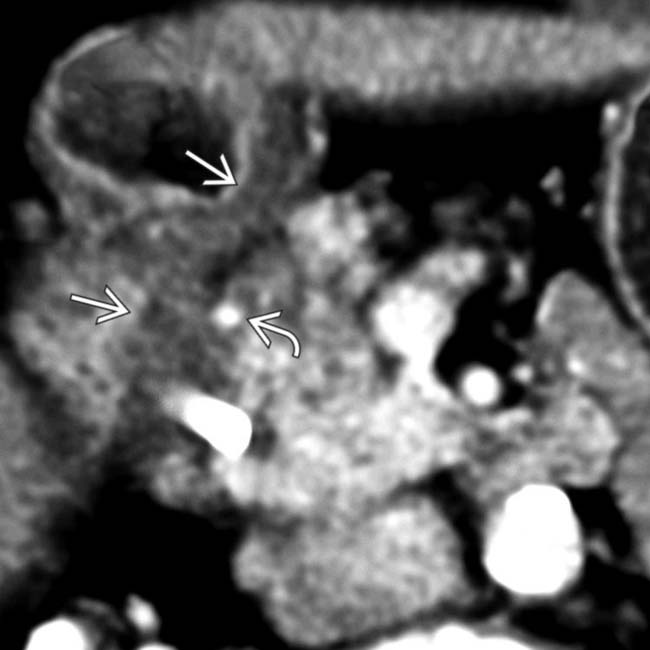
 and thickens the medial wall of the 2nd duodenum
and thickens the medial wall of the 2nd duodenum  .
.