• Overall prognosis for CF has dramatically improved, with average life expectancy now 35-40 years
• Respiratory failure most common cause of mortality, with liver disease 2nd leading cause of death
• Pancreatic insufficiency most common (∼ 85%) GI manifestation of CF
(Left) Axial CECT shows the classic lipomatous replacement and pseudohypertrophy of the pancreas in a young adult patient with cystic fibrosis (CF).
(Right) Axial CECT in the same patient shows dilated proximal small bowel and collapsed distal small bowel . Just proximal to the point of transition is the classic “small bowel feces sign” associated with mechanical small-bowel obstruction, with the obstruction caused by inspissated enteric contents (distal intestinal obstruction syndrome or DIOS).
(Left) Axial CECT demonstrates heterogeneous lipomatous replacement of the pancreatic parenchyma but less pseudohypertrophy. This 29-year-old woman had longstanding pancreatic exocrine dysfunction due to CF.
(Right) Coronal CECT demonstrates simple-appearing cysts in the pancreatic head in a young patient with CF. While pancreatic cysts are often very small in CF patients, they can rarely be larger, as in this case.
TERMINOLOGY
Abbreviations
• Cystic fibrosis (CF)
Synonyms
• Mucoviscidosis
Definitions
• Recessively inherited disorder of epithelial chloride transport caused by mutation of CF transmembrane conductance regulator (CFTR) gene
Pulmonary manifestations are primary cause of morbidity and mortality
CF increasingly seen to affect GI tract due to improved life expectancy
IMAGING
General Features
• Best diagnostic clue
Diffuse fatty replacement of pancreas is most common abdominal imaging finding
• Location
Most common sites of involvement are lungs, pancreas, bowel, liver, and exocrine glands
CT Findings
• Pancreatic manifestations
Early childhood: Heterogeneous attenuation of pancreas
Later childhood: Complete fatty replacement of parenchyma (often by teenage years)
Pancreatic cysts: Usually simple in appearance
– Related to inspissated secretions which lead to ductal obstruction
– Cysts are usually small (< 3 mm), but can be larger
– Cysts may diffusely replace pancreas (cystosis)
– Usually occur in patients in their 20s, and may be symptomatic as result of cyst hemorrhage
Repeated episodes of acute pancreatitis with development of chronic pancreatitis
– Pancreatic ductal strictures, dilatation, beading, etc.
May have scattered calcifications (< 10% of patients)
Increased risk of pancreatic cancer (very rare)
MR Findings
• Enlarged pancreas with diffuse fatty infiltration appears hyperintense on T1WI
• Pancreas can also appear abnormally hypointense on T1WI due to chronic pancreatitis and fibrosis
• Pancreatic cysts well demonstrated on T2WI and MRCP (hyperintense)
• Pancreatic duct abnormalities also occasionally seen
Ultrasonographic Findings
• Pancreas may be barely identifiable as result of diffuse fibrofatty replacement
• Macroscopic multiple cysts
• Hypoechoic enlargement of pancreas noted in some children with acute pancreatitis
Other Abdominal Findings
• Liver
30-50% develop hepatic steatosis ± hepatomegaly
– Can be visualized with US, CT, or chemical shift MR
– Fatty liver usually asymptomatic and does not correlate with development of CF-related cirrhosis
Cirrhosis in 5-15% of all CF patients with portal hypertension in 1-8%
Gallstones in up to 1/4 of patients with CF, often with nonspecific gallbladder wall thickening and sludge
Microgallbladder in 30% of CF patients at autopsy
– Probably due to chronic stenosis or atresia of cystic duct (does not usually cause symptoms)
May develop bile duct abnormalities very similar to primary sclerosing cholangitis (PSC), including strictures, bile duct wall thickening, biliary obstruction, etc.
– May develop focal biliary fibrosis (> 3/4 of patients with CF older than 24 years)
Periductal thickening and fibrosis due to thick secretions within duct and reactive inflammation
Focal thickening of bile duct with changes in adjacent liver parenchymal density/signal
US: Hyperechoic periportal thickening and diffuse hepatic hyperechogenicity
– MRCP best noninvasive modality for identifying changes
• Esophagus
Gastroesophageal (GE) reflux seen in 27% of patients younger than 5 years and increases with age
Complications detected with esophagram or endoscopy
• Bowel
↑ frequency of peptic ulcer disease (gastric or duodenal)
Obstruction
– Bubbly fecal mass within bowel causing proximal obstruction, most often in infants (meconium ileus)
– Obstruction can also occur in adults: Distal intestinal obstruction syndrome (DIOS) (previously known as meconium ileus equivalent)
Obstruction results from thickened intestinal secretions, poor motility, and formation of mass-like fecal material which obstructs bowel
Usually obstructs at distal ileum or right colon (rarely at distal rectum)
Water-soluble contrast enema might be able to reduce obstruction
Increased risk for intussusception
– More common in older patients
– Most often ileocolic intussusception, usually due to inspissated fecal material acting as lead point
– US: “Doughnut” or pseudokidney appearance
– CT: “Target” sign of edematous bowel and intermixed mesenteric fat
– Water-soluble contrast enema can be used for reduction, but high rates of recurrence
Chronically distended appendix common with internal inspissated high-density material
– Differentiating acute appendicitis from chronic distention is difficult with imaging
– Appendicitis in 1-4% of patients
Abnormalities of colon can include proximal colonic wall thickening, proliferation of fat surrounding the colon, and pericolonic fat stranding
– Benign pneumatosis due to air dissecting below diaphragm into bowel wall due to lung disease
– Increased susceptibility to pseudomembranous colitis
– Increased risk of colon cancer
– Rectal mucosal prolapse usually in younger patients
20% of patients with CF
• Renal
Nephrolithiasis in 3-6% CF patients
Interstitial nephritis due to antibiotics and amyloidosis will likely become more common as patients live longer
DIFFERENTIAL DIAGNOSIS
Pancreatic Lipomatous Pseudohypertrophy
• Diffuse enlargement and fatty replacement of pancreas
• Associated with chronic liver disease; no signs of CF
Shwachman-Diamond Syndrome
• Pancreatic lipomatosis associated with short stature
• Appearance of pancreas is identical to CF
Normal Fatty Lobulation
• Fatty replacement of pancreatic parenchyma with mild glandular atrophy
• Common in elderly, obese, and diabetic patients
Chronic Pancreatitis
• Pancreatic atrophy, parenchymal and ductal calcifications, and pancreatic ductal beading, irregularity, and dilatation
• Pancreatic volume is usually decreased
May have focal soft tissue density enlargement (usually in head)
• Intra- or peripancreatic cysts
• Pancreatic findings may mimic CF, but lacks other clinical signs
Pancreatic Cystic Neoplasms (IPMN, etc.)
• May be indistinguishable from CF-related pancreatic cysts without clinical history
PATHOLOGY
General Features
• Etiology
Mutations of CFTR gene lead to multisystem pathology
Disruption of chloride ion, bicarbonate, and water transport in duct cells
Pancreatic insufficiency usually present from birth
– Repetitive acute pancreatitis leading to chronic pancreatitis
Susceptible to infection by Staphylococcus aureus and Pseudomonas aeruginosa
Pancreatitis in 10% of CF patients
– Endocrine (diabetes) and exocrine dysfunction
Symptoms of hepatobiliary dysfunction
– Inspissated secretions obstruct bile ducts and caustic bile acts on adjacent parenchyma
– Liver disease can vary from asymptomatic elevation in liver function tests to end-stage liver disease and cirrhosis
– 10-20% of patients develop chronic liver disease (including cirrhosis and portal hypertension)
– Cholelithiasis in 10% of patients
Intestinal manifestations
– Intestinal obstruction
Usually in infancy (meconium ileus), but may occur in adults as well (DIOS or meconium ileus equivalent)
– Intussusceptions (1% of patients)
Infertility in males (azoospermia, turbid semen)
Demographics
• Age
Children most affected
Patients reaching adulthood represent rapidly growing percentage of CF population
• Ethnicity
More common in Caucasians
– Most common inherited fatal disease in Caucasians
• Epidemiology
CF prevalence: 1 in 3,500
85–90% of CF patients have pancreatic exocrine gland insufficiency
– Cystic fibrosis is major cause of pancreatic exocrine failure in childhood
30-50% of CF patients have pancreatic endocrine gland dysfunction
Natural History & Prognosis
• Overall prognosis for CF has dramatically improved due to screening and better treatment, with average life expectancy now 35-40 years
• Respiratory failure most common cause of mortality
Liver disease is 2nd leading cause of death
– Liver disease increasingly being seen as CF life expectancy increases
• Pancreatic insufficiency most common (∼ 85%) GI manifestation of CF
Varies depending on degree of ductal obstruction by mucus, which leads to exocrine gland atrophy, progressive fibrosis, and cyst formation
CF may predispose to pancreatic cancer
Treatment
• Aggressive nutritional and pancreatic enzyme therapy
• DIOS usually treatable with hydration, laxatives, or water soluble contrast enema although severe cases may require surgery
(Left) Axial CT image shows diffuse pneumatosis of the transverse and left colon. The patient was completely asymptomatic, and this was felt to be benign pneumatosis due to gas dissecting from the chest into the bowel wall as a result of the patient’s lung disease.
(Right) Axial NECT in a 24-year-old woman with CF shows an unusually severe degree of pancreatic calcification . Scattered, small calcifications are a more common finding in this disease.
(Left) Axial T2WI in a 16-year-old girl with CF demonstrates complete fatty replacement of the body and tail of the pancreas. Note that the pancreas consequently shows high T1WI signal.
(Right) Coronal MRCP in the same patient shows a septate cystic mass in the pancreatic head that mimics a cystic neoplasm. However, pancreatic cysts of variable size are commonly encountered in patients with CF.
(Left) Axial CECT in a 31-year-old man shows classic cystic bronchiectasis in the lungs. Many patients are being kept alive longer with better medical care and even lung transplantation, resulting in an increased prevalence of extrapulmonary manifestations of CF.
(Right) Axial CECT in the same patient shows that the liver is small and cirrhotic with obvious signs of portal hypertension, including splenomegaly and large varices . The pancreas shows fatty replacement .
Axial NECT shows lipomatous replacement of the entire pancreas.
Axial NECT shows lipomatous replacement and pseudohypertrophy of entire pancreas.
Axial NECT shows hyperaeration of the upper lobes with cystic bronchiectasis in a patient with CF.
Axial CECT shows lipomatous replacement of the pancreas and 1 of several small cysts .
Coronal CECT demonstrates a simple-appearing cyst in the pancreatic tail in a young patient with CF. Notice the fatty infiltration of the surrounding pancreatic tail. While pancreatic cysts are often very small in CF patients, they can rarely be larger, as in this case.
Axial CT image demonstrates diffuse pneumatosis in the rectum. The patient was completely asymptomatic, and this was felt to be benign pneumatosis due to gas dissecting from the chest into the bowel wall as a result of the patient’s lung disease.
Axial CECT in a young adult with cystic fibrosis shows a moderate degree of lipomatous pseudohypertrophy of the pancreas . The pancreatic duct is of normal caliber .
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Complete fatty infiltration and replacement of parenchyma (often by end of teenage years)
Pancreatic cysts: Usually small (< 3 mm), but can be larger and can completely replace pancreas (cystosis)
Repeated episodes of acute pancreatitis with development of chronic pancreatitis
• Liver
30-50% develop hepatic steatosis ± hepatomegaly
Can develop multinodular cirrhosis in severe cases
• Biliary
Biliary abnormalities similar to primary sclerosing cholangitis (PSC)
Gallstones ± gallbladder wall thickening and sludge
• Bowel
Inspissated fecal material resulting in proximal obstruction, most often in infants (meconium ileus)
Obstruction can also occur in adults: Distal intestinal obstruction syndrome (DIOS)
Increased risk for intussusception
Chronically distended appendix may be difficult to distinguish from acute appendicitis
• Overall prognosis for CF has dramatically improved, with average life expectancy now 35-40 years
• Respiratory failure most common cause of mortality, with liver disease 2nd leading cause of death
• Pancreatic insufficiency most common (∼ 85%) GI manifestation of CF
(Left) Axial CECT shows the classic lipomatous replacement and pseudohypertrophy of the pancreas in a young adult patient with cystic fibrosis (CF).
(Right) Axial CECT in the same patient shows dilated proximal small bowel and collapsed distal small bowel . Just proximal to the point of transition is the classic “small bowel feces sign” associated with mechanical small-bowel obstruction, with the obstruction caused by inspissated enteric contents (distal intestinal obstruction syndrome or DIOS).
(Left) Axial CECT demonstrates heterogeneous lipomatous replacement of the pancreatic parenchyma but less pseudohypertrophy. This 29-year-old woman had longstanding pancreatic exocrine dysfunction due to CF.
(Right) Coronal CECT demonstrates simple-appearing cysts in the pancreatic head in a young patient with CF. While pancreatic cysts are often very small in CF patients, they can rarely be larger, as in this case.
TERMINOLOGY
Abbreviations
• Cystic fibrosis (CF)
Synonyms
• Mucoviscidosis
Definitions
• Recessively inherited disorder of epithelial chloride transport caused by mutation of CF transmembrane conductance regulator (CFTR) gene
Pulmonary manifestations are primary cause of morbidity and mortality
CF increasingly seen to affect GI tract due to improved life expectancy
IMAGING
General Features
• Best diagnostic clue
Diffuse fatty replacement of pancreas is most common abdominal imaging finding
• Location
Most common sites of involvement are lungs, pancreas, bowel, liver, and exocrine glands
CT Findings
• Pancreatic manifestations
Early childhood: Heterogeneous attenuation of pancreas
Later childhood: Complete fatty replacement of parenchyma (often by teenage years)
Pancreatic cysts: Usually simple in appearance
– Related to inspissated secretions which lead to ductal obstruction
– Cysts are usually small (< 3 mm), but can be larger
– Cysts may diffusely replace pancreas (cystosis)
– Usually occur in patients in their 20s, and may be symptomatic as result of cyst hemorrhage
Repeated episodes of acute pancreatitis with development of chronic pancreatitis
– Pancreatic ductal strictures, dilatation, beading, etc.
May have scattered calcifications (< 10% of patients)
Increased risk of pancreatic cancer (very rare)
MR Findings
• Enlarged pancreas with diffuse fatty infiltration appears hyperintense on T1WI
• Pancreas can also appear abnormally hypointense on T1WI due to chronic pancreatitis and fibrosis
• Pancreatic cysts well demonstrated on T2WI and MRCP (hyperintense)
• Pancreatic duct abnormalities also occasionally seen
Ultrasonographic Findings
• Pancreas may be barely identifiable as result of diffuse fibrofatty replacement
• Macroscopic multiple cysts
• Hypoechoic enlargement of pancreas noted in some children with acute pancreatitis
Other Abdominal Findings
• Liver
30-50% develop hepatic steatosis ± hepatomegaly
– Can be visualized with US, CT, or chemical shift MR
– Fatty liver usually asymptomatic and does not correlate with development of CF-related cirrhosis
Cirrhosis in 5-15% of all CF patients with portal hypertension in 1-8%
 Pancreatic cysts: Usually small (< 3 mm), but can be larger and can completely replace pancreas (cystosis)
Pancreatic cysts: Usually small (< 3 mm), but can be larger and can completely replace pancreas (cystosis)









 in a young adult patient with cystic fibrosis (CF).
in a young adult patient with cystic fibrosis (CF).
 and collapsed distal small bowel
and collapsed distal small bowel  . Just proximal to the point of transition is the classic “small bowel feces sign”
. Just proximal to the point of transition is the classic “small bowel feces sign”  associated with mechanical small-bowel obstruction, with the obstruction caused by inspissated enteric contents (distal intestinal obstruction syndrome or DIOS).
associated with mechanical small-bowel obstruction, with the obstruction caused by inspissated enteric contents (distal intestinal obstruction syndrome or DIOS).
 but less pseudohypertrophy. This 29-year-old woman had longstanding pancreatic exocrine dysfunction due to CF.
but less pseudohypertrophy. This 29-year-old woman had longstanding pancreatic exocrine dysfunction due to CF.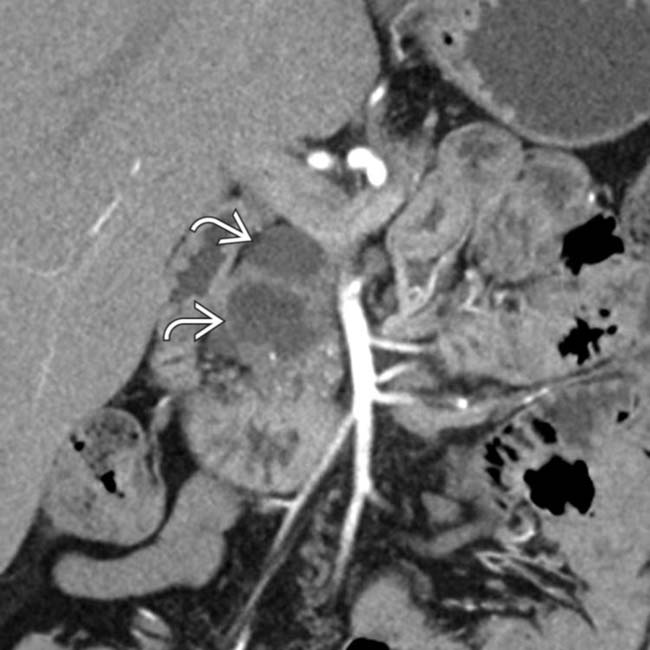
 in the pancreatic head in a young patient with CF. While pancreatic cysts are often very small in CF patients, they can rarely be larger, as in this case.
in the pancreatic head in a young patient with CF. While pancreatic cysts are often very small in CF patients, they can rarely be larger, as in this case.












 Gallstones in up to 1/4 of patients with CF, often with nonspecific gallbladder wall thickening and sludge
Gallstones in up to 1/4 of patients with CF, often with nonspecific gallbladder wall thickening and sludge







 Obstruction
Obstruction
 Increased risk for intussusception
Increased risk for intussusception















 Symptoms of hepatobiliary dysfunction
Symptoms of hepatobiliary dysfunction




















 of the transverse and left colon. The patient was completely asymptomatic, and this was felt to be benign pneumatosis due to gas dissecting from the chest into the bowel wall as a result of the patient’s lung disease.
of the transverse and left colon. The patient was completely asymptomatic, and this was felt to be benign pneumatosis due to gas dissecting from the chest into the bowel wall as a result of the patient’s lung disease.
 . Scattered, small calcifications are a more common finding in this disease.
. Scattered, small calcifications are a more common finding in this disease.
 of the body and tail of the pancreas. Note that the pancreas consequently shows high T1WI signal.
of the body and tail of the pancreas. Note that the pancreas consequently shows high T1WI signal.
 that mimics a cystic neoplasm. However, pancreatic cysts of variable size are commonly encountered in patients with CF.
that mimics a cystic neoplasm. However, pancreatic cysts of variable size are commonly encountered in patients with CF.

 . The pancreas shows fatty replacement
. The pancreas shows fatty replacement  .
.



 .
.
 in the pancreatic tail in a young patient with CF. Notice the fatty infiltration of the surrounding pancreatic tail. While pancreatic cysts are often very small in CF patients, they can rarely be larger, as in this case.
in the pancreatic tail in a young patient with CF. Notice the fatty infiltration of the surrounding pancreatic tail. While pancreatic cysts are often very small in CF patients, they can rarely be larger, as in this case.

 . The pancreatic duct is of normal caliber
. The pancreatic duct is of normal caliber  .
.