[level-membership-for-radiology-category] Well defined/lobulated or poorly marginated

 Pancreatic duct (PD) obstructed in only ∼ 50%, and usually does not cause upstream pancreatic atrophy
Pancreatic duct (PD) obstructed in only ∼ 50%, and usually does not cause upstream pancreatic atrophy

PATHOLOGY
• Lesions can be divided into 3 forms
 Tumors arising from duodenal epithelium (intestinal type): Prognosis comparable to duodenal carcinoma
Tumors arising from duodenal epithelium (intestinal type): Prognosis comparable to duodenal carcinoma
Tumors arising from duodenal epithelium (intestinal type): Prognosis comparable to duodenal carcinoma

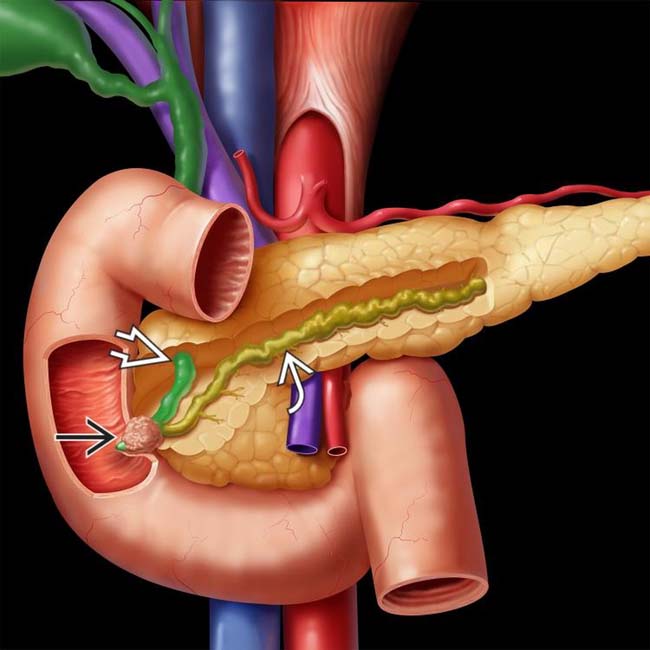
 causing obstruction of both the common bile duct (CBD)
causing obstruction of both the common bile duct (CBD)  and the pancreatic duct (PD)
and the pancreatic duct (PD)  .
.
 causing obstruction of the distal common duct at the ampulla. Patients with familial polyposis have a substantially increased risk of developing ampullary (and other) carcinomas. Lifelong surveillance is required to detect bowel, stomach, and biliary tumors.
causing obstruction of the distal common duct at the ampulla. Patients with familial polyposis have a substantially increased risk of developing ampullary (and other) carcinomas. Lifelong surveillance is required to detect bowel, stomach, and biliary tumors.
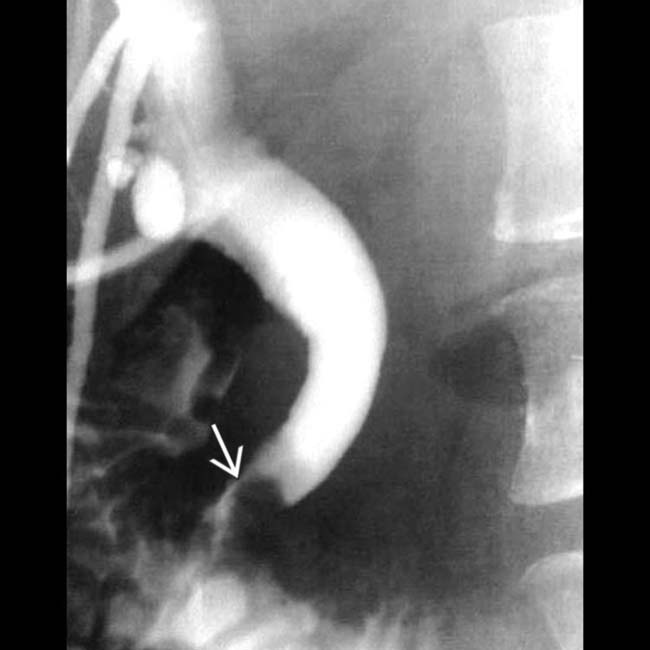
 , with obstruction of both the common bile duct
, with obstruction of both the common bile duct  and pancreatic duct
and pancreatic duct  . Note the abrupt occlusion of both ducts by the mass.
. Note the abrupt occlusion of both ducts by the mass.
 centered at the ampulla obstructing the pancreatic and common bile ducts. While this was a pancreaticobiliary type lesion at histology, individual subtypes of ampullary carcinoma cannot be distinguished on imaging.
centered at the ampulla obstructing the pancreatic and common bile ducts. While this was a pancreaticobiliary type lesion at histology, individual subtypes of ampullary carcinoma cannot be distinguished on imaging.IMAGING
General Features

























PATHOLOGY
General Features
• Etiology

































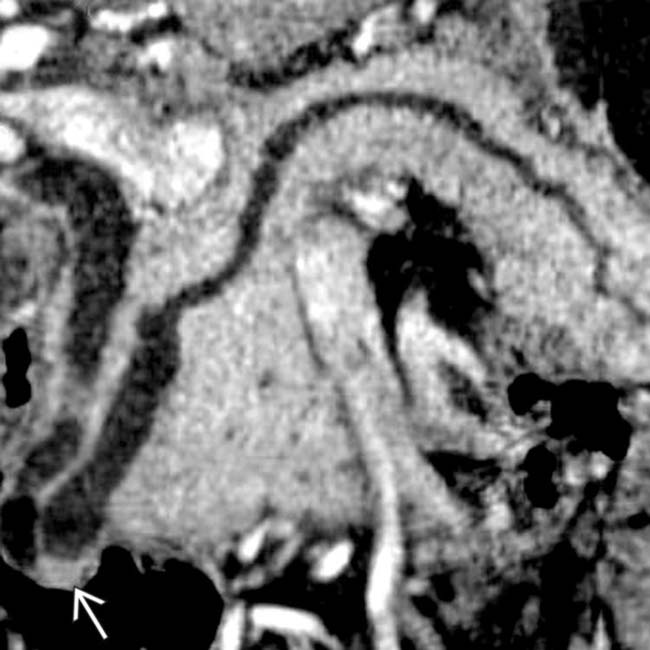
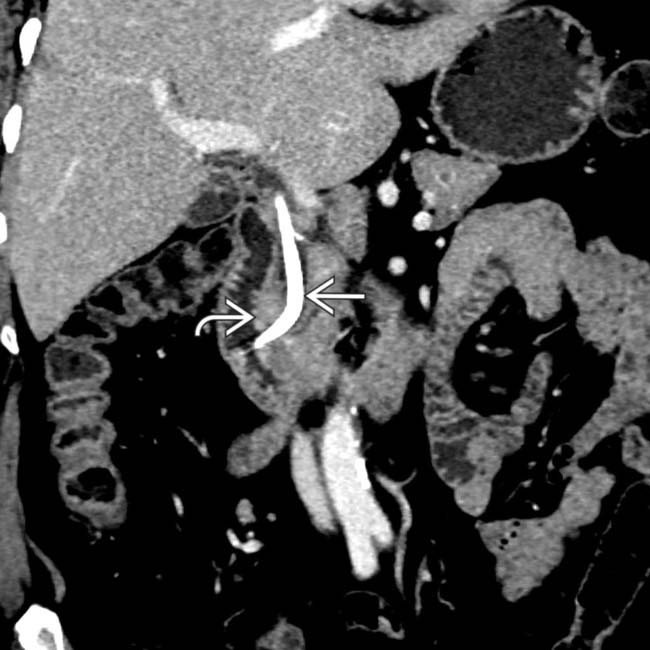
 centered at the ampulla, representing an ampullary carcinoma. A biliary stent
centered at the ampulla, representing an ampullary carcinoma. A biliary stent  is partially visualized. The coronal plane is usually the best way of visualizing the ampulla and assessing a potential mass.
is partially visualized. The coronal plane is usually the best way of visualizing the ampulla and assessing a potential mass.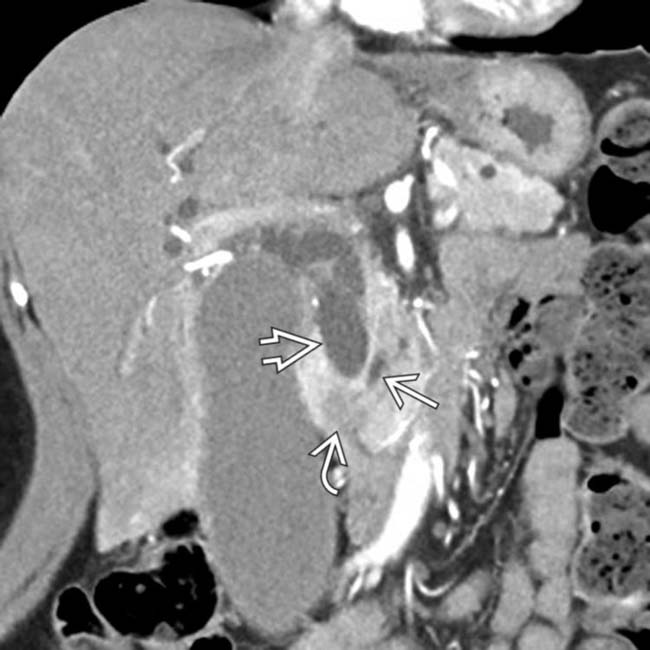
 obstructing the common bile duct
obstructing the common bile duct  , with only mild dilatation of the pancreatic duct
, with only mild dilatation of the pancreatic duct  . This was found to represent an ampullary carcinoma at surgery.
. This was found to represent an ampullary carcinoma at surgery.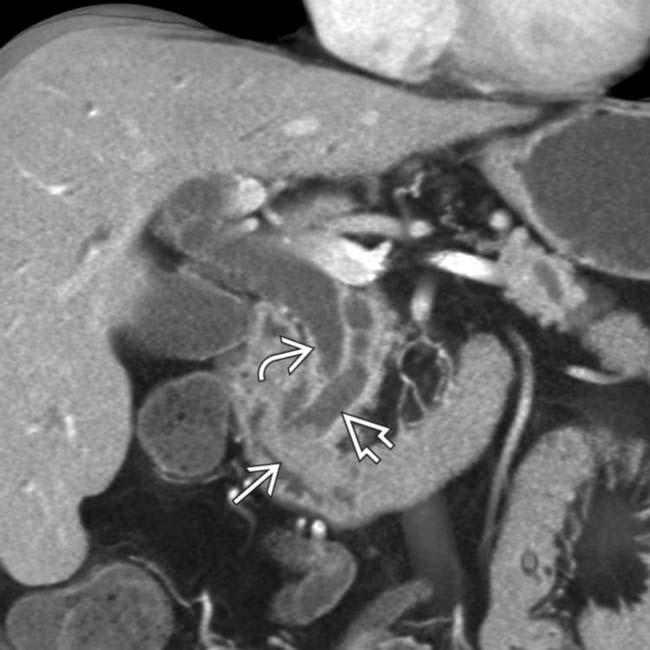
 and pancreatic duct
and pancreatic duct  by a polypoid ampullary carcinoma
by a polypoid ampullary carcinoma  .
.
 centered around the ampulla with a biliary stent
centered around the ampulla with a biliary stent  . Ampullary carcinoma cannot be easily distinguished from a periampullary duodenal carcinoma at imaging, although surgical treatment for both lesions is the same (Whipple procedure).
. Ampullary carcinoma cannot be easily distinguished from a periampullary duodenal carcinoma at imaging, although surgical treatment for both lesions is the same (Whipple procedure).
 obstructing the CBD
obstructing the CBD  . The PD (not shown) was not obstructed. Ampullary carcinomas almost always obstruct the CBD, but obstruct the PD in only 50% of cases.
. The PD (not shown) was not obstructed. Ampullary carcinomas almost always obstruct the CBD, but obstruct the PD in only 50% of cases.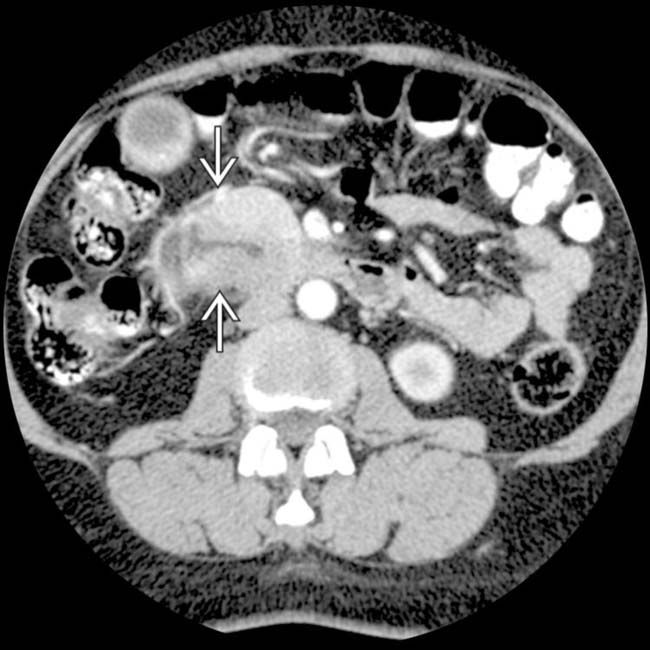
 at the junction of the 2nd and 3rd portions of the duodenum.
at the junction of the 2nd and 3rd portions of the duodenum.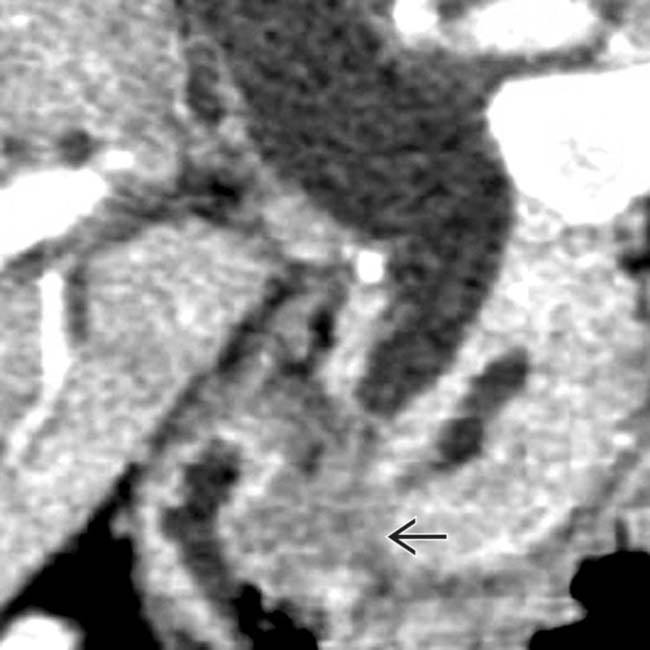
 obstructing the pancreatic and common bile ducts.
obstructing the pancreatic and common bile ducts.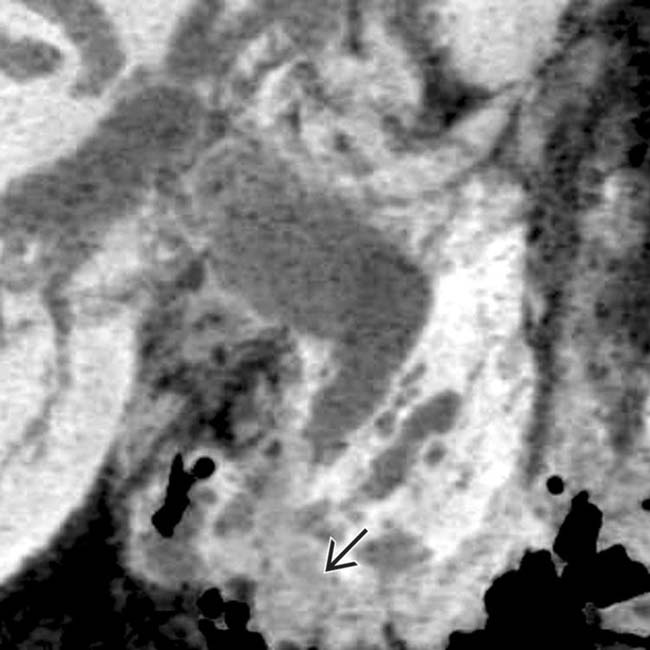
 .
.
 .
.
 obstructing the pancreatic and common bile ducts.
obstructing the pancreatic and common bile ducts.
 with an unusual degree of increased vascularity.
with an unusual degree of increased vascularity.
 .
.
 centered in the duodenum at the level of the ampulla, found to represent an ampullary carcinoma at histology. Note the presence of a biliary stent
centered in the duodenum at the level of the ampulla, found to represent an ampullary carcinoma at histology. Note the presence of a biliary stent  due to biliary obstruction by the mass.
due to biliary obstruction by the mass.[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Well defined/lobulated or poorly marginated
Pancreatic duct (PD) obstructed in only ∼ 50%, and usually does not cause upstream pancreatic atrophyPATHOLOGY
• Lesions can be divided into 3 forms
Tumors arising from duodenal epithelium (intestinal type): Prognosis comparable to duodenal carcinoma
Tumors arising from duodenal epithelium (intestinal type): Prognosis comparable to duodenal carcinoma causing obstruction of both the common bile duct (CBD) and the pancreatic duct (PD) . causing obstruction of the distal common duct at the ampulla. Patients with familial polyposis have a substantially increased risk of developing ampullary (and other) carcinomas. Lifelong surveillance is required to detect bowel, stomach, and biliary tumors., with obstruction of both the common bile duct and pancreatic duct . Note the abrupt occlusion of both ducts by the mass. centered at the ampulla obstructing the pancreatic and common bile ducts. While this was a pancreaticobiliary type lesion at histology, individual subtypes of ampullary carcinoma cannot be distinguished on imaging.IMAGING
General Features
Imaging Recommendations
• Protocol advice
 Patients drink 500 cc water immediately prior to CT to distend duodenum (improving visualization of ampulla)
Patients drink 500 cc water immediately prior to CT to distend duodenum (improving visualization of ampulla)
Patients drink 500 cc water immediately prior to CT to distend duodenum (improving visualization of ampulla)Buy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
