[level-membership-for-orthopaedics-category]38
Mechanical disorders of the lumbar spine
Differential diagnosis



Box 38.2 Backache
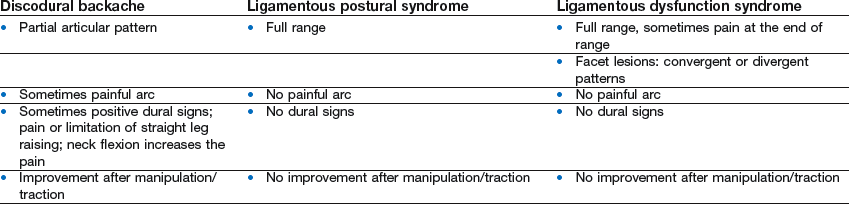
• Acute and recurrent backache: almost always caused by a discodural interaction, thus symptoms and signs are very similar to acute lumbago, although milder. Dural symptoms and signs are sometimes subtle or even absent. A clear non-capsular pattern or a painful arc during flexion is pathognomonic for a small central disc protrusion
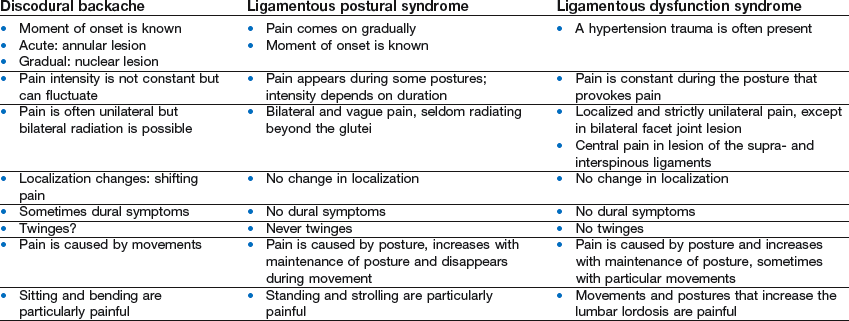
• Chronic backache: caused by either a discodural interaction or a lesion of a posterior structure (facet or ligament)


Box 38.3 Sciatica
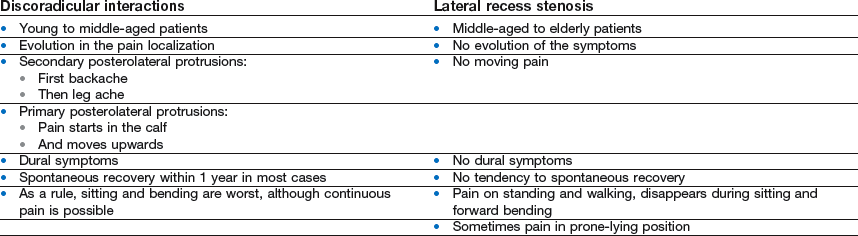
• Radicular compression can result either from a posterolateral disc herniation or from a narrowed lateral recess
• Discoradicular conflicts have a typical age of onset and typical natural history
• Entrapment of the nerve root in the lateral recess occurs in elderly patients; there is virtually no spontaneous evolution





[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]38
Mechanical disorders of the lumbar spine
Differential diagnosis
