CASE 20
A 38-year-old female, MM, is seen in your office complaining of malaise for the past several months, a chronic cough, and pain in the left flank with hematuria (red blood cells in the urine). There is no medical history of note. There is no recent travel; she is afebrile, a nonsmoker, and not on any medication (either over-the-counter or prescribed). There is a family history of kidney stones, but her diet is not particularly rich in proteins, oxalates, or dairy products.
QUESTIONS FOR GROUP DISCUSSION
RECOMMENDED APPROACH
Implications/Analysis of Family History
A familial history of kidney stones in a female directs us away from any X-linked disorders.
Implications/Analysis of Clinical History
The hematuria, combined with MM’s family history, is suggestive of renal colic (intense pain in the lower back on one side as a result of passing a small stone down the ureter). But, if this is the problem, what is causing the kidney stone formation? Of note is the fact that both the lungs and kidneys are affected. We have already encountered two autoimmune diseases, Goodpasture’s syndrome (see Case 17) and systemic lupus erythematosus (see Case 18), that cause a similar type of presentation owing to immune complex deposition in these tissues. Some drug-induced allergies can also manifest like this.
Additional Laboratory Tests
Pulmonary Function Tests
A spirometer is used to measure how rapidly a person can blow air out of the lungs following deep inhalation. Another lung test measures how much air the lung can hold (lung volume). (See Case 19.) Both of these were lower than normal when MM was tested, which is consistent with a diagnosis of sarcoidosis.
Kviem Test
This is a skin test, similar to the Mantoux test, in that it involves the subcutaneous injection of a substance and examination 48 hours later. In the Kviem test, which was developed in the late 1930s, a spleen homogenate from a person with sarcoidosis is injected intradermally into the person suspected of having sarcoidosis. Although a positive result can be seen after 48 hours, the area is not sampled for 4 to 6 weeks to allow time for granuloma formation. Formation of a noncaseating granuloma supports a diagnosis of sarcoidosis. A positive result is obtained in about 80% of all patients with active sarcoidosis (50% nonactive disease) but less than 1% of the normal population. This test is not FDA approved, nor has it been standardized.
ETIOLOGY: SARCOIDOSIS
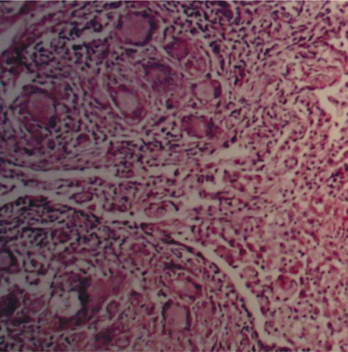
Sarcoidosis is a multisystemic disease of unknown etiology that may affect any organ in the body. However, most patients have some degree of lung involvement. The highest incidence of the disease occurs in young African American males. Sarcoidosis is a type IV hypersensitivity reaction, precipitated by chronic Th1 sensitization/activation in response to ill-defined antigens, leading (as in tuberculosis) to chronic granuloma formation. A granuloma consists of an aggregate of cells arranged in almost concentric layers focused about macrophage-derived epithelioid cells (so named because histologically they resemble epithelial cells). Giant cells resulting from the fusion of macrophages may be present. Lymphocytes surround this region (Fig. 20-1). Older granulomas develop a circle of fibroblasts that define the outer region along with fibrous connective tissue.