Topic 2 Evaluation of myocardial ischaemia
Markers of myocardial injury and infarction
A universal classification system for myocardial infarction (MI) was published in 2007.
Troponin values may remain elevated for 7–14 days following the onset of infarction.
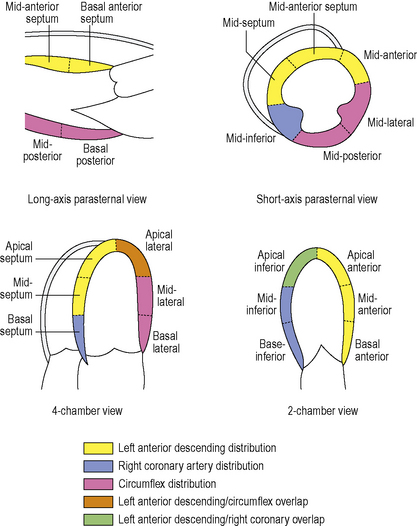
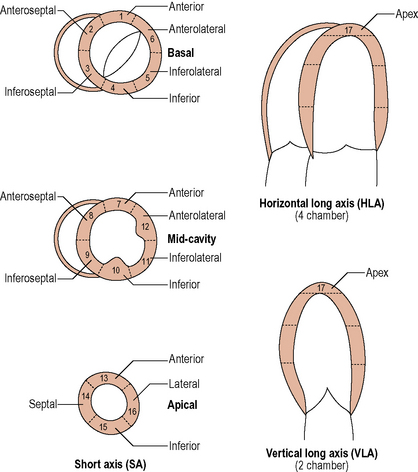
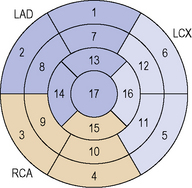
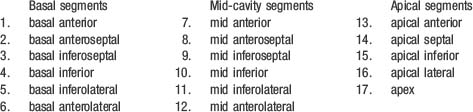
The 17 segment model (see Figure 2.2)
Stress tests
Exercise ECG stress test
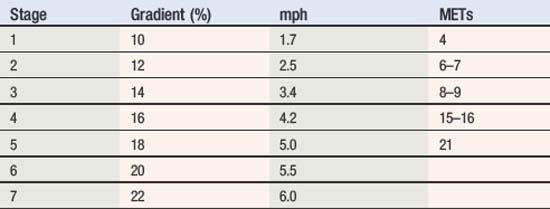
Various standardized protocols are available. The Bruce Protocol is commonly used (Table 2.1).
Nuclear imaging
Single photon emission computed tomography (SPECT)
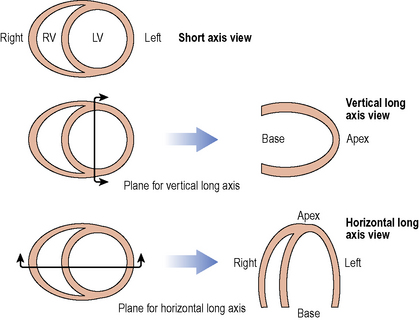
SPECT describes the use of a rotating gamma camera, which enables reconstruction to create a three dimensional image. Standard views are shown in Figure 2.4.
Positron emission tomography
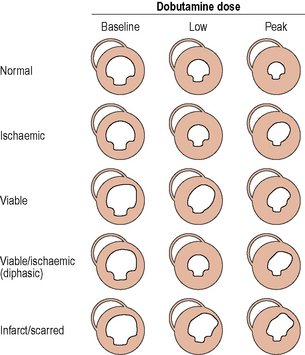
Stress echocardiography
Typical pharmacological agents: dobutamine (+/– atropine), adenosine, dipyridamole.
The dobutamine dose is 5–10 µg/kg/min increased in increments to max 40 µg/kg/min.
Atropine can be given in addition to increase heart rate to target.
A number can be assigned to each segment and a wall motion score can be calculated:
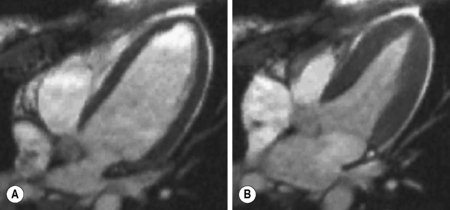
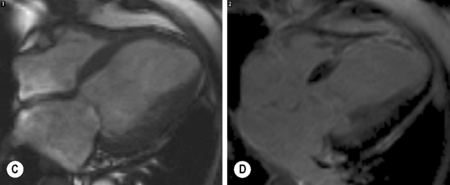
Cardiac magnetic resonance imaging (see Figure 2.6)
Techniques used in the assessment of coronary artery disease include the following:
Coronary calcification imaging
Coronary artery calcification occurs almost exclusively in atherosclerosis. Detection of calcium with CT is used to assess plaque burden. This has been translated into a calcium score: Agatston score (Table 2.2). The score is generated from the product of calcium plaque area and calcium plaque density (Hounsfield number).
Table 2.2 Description of plaque burden according to calcium score
| 0 | No identifiable atherosclerotic plaque |
| 1–10 | Minimal plaque burden |
| 11–100 | Mild plaque burden |
| 101–400 | Moderate plaque burden |
| Over 400 | Extensive plaque burden |
The absolute value can also be matched against expected score for age.
Diagnostic adjuncts in angiography and percutaneous intervention
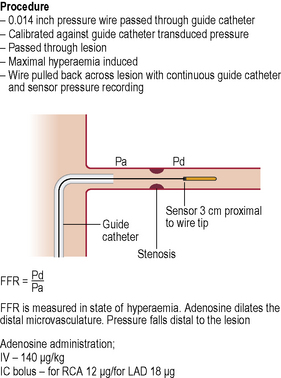
Pressure wire
The pressure wire study allows physiological assessment of coronary lesions (Figure 2.7).