CASE 196
History: A 62-year-old man presents with a 4-day history of nausea and vomiting with a palpable mass in the right iliac fossa.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. What is the most common etiology for superior mesenteric venous occlusion?
3. What is the most specific imaging sign of superior mesenteric venous thrombosis?
C. Superior mesenteric vein filling defect
D. Portal venous cavernous transformation
4. What part of the gastrointestinal tract would you anticipate would be most severely affected by superior mesenteric venous occlusion?
C. Small bowel and ascending colon
D. Descending and sigmoid colon
ANSWERS
CASE 196
Superior Mesenteric Venous Occlusion
1. A, B, C, and E
2. A
3. C
4. C
References
Bradbury MS, Kavanagh PV, Bechtold RE, et al: Mesenteric venous thrombosis: diagnosis and noninvasive imaging. Radiographics. 2002;22(3):527-541.
Kumar S, Sarr MG, Kamath PS. Mesenteric venous thrombosis. N Engl J Med. 2001;345(23):1683-1688.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 144.
Comment
Mesenteric venous thrombosis is an uncommon form of mesenteric ischemia and infarction. This condition, with a mortality rate of 30% to 40%, is seen in patients with hypercoagulable states, such as intraabdominal sepsis, pregnancy, and polycythemia vera, and in some women taking oral contraceptives. A few cases have been reported in pregnant women who have accidentally taken oral contraceptives. Other wide-ranging causes include blunt trauma and certain malignancies; rarely, it is seen after abdominal surgeries.
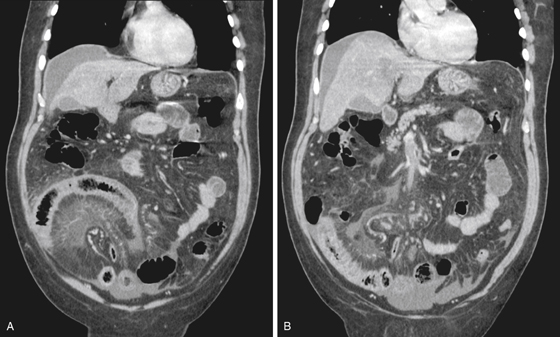
The striking findings in this case are the segmental distribution of marked small bowel abnormality (see figures), including congestion in the mesentery, and the filling defect within the lumen of the superior mesenteric vein (see figures). There is also free fluid in the abdomen, which can be expected in this condition. The high mortality rate associated with this condition is most likely due to the prolonged time of seeking medical attention and delayed diagnosis.






