CASE 192
History: A 33-year-old woman presents with epigastric pain and vomiting.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
E. Hypertrophic pyloric stenosis
2. What is the eponym for a penetrating ulcer that extends from the distal gastric antrum to the base of the duodenum, paralleling the pyloric channel?
3. What is the most common complication of peptic ulceration?
4. Which of the following radiographic signs would be most useful in diagnosing a lesion seen on a barium upper GI study as a polyp rather than a diverticulum?
B. Lesion location in the fundus
C. Filling defect in the barium pool
D. Bowler hat sign pointing outward
ANSWERS
CASE 192
Pyloric Channel Ulcer
1. A, B, C, and D
2. C
3. A
4. C
References
Levine MS. Peptic ulcers. In: Gore RM, Levine MS, eds. Textbook of Gastrointestinal Radiology. 2nd ed Philadelphia: Saunders; 2000:514-545.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 97.
Comment
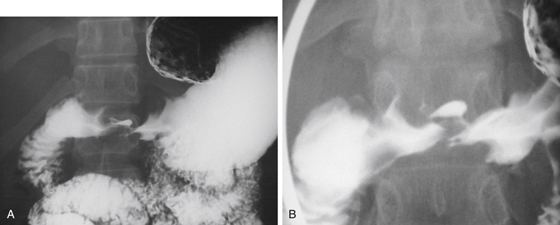
This upper GI double-contrast barium examination clearly shows a persistent collection of barium in the pyloric channel (see figures). Ulcers collect barium because they are essentially holes in the mucosa. An ulcer collects barium in the same manner in which a pothole in the road may collect water. The granulation tissue that forms the base of the ulceration tends to cause the barium to become adherent to the ulcer crater. Diverticula also collect barium in the same manner. Space-occupying lesions such as polyps and masses displace barium, which is called a filling defect.
Although this was basic knowledge a decade ago, it seems less basic to current residents. The widespread use of endoscopy and decreased number of upper GI examinations done by radiologists and the great interest in newer modalities seem to have relegated expertise in barium procedures to a small niche in the radiology department of the 21st century. Nevertheless, the examinations are still relevant, and radiologists are still required to have some basic knowledge. Dragsted, who connected hyperacidity to peptic disease (although to some extent this had been done by Beaumont in 1835), was a surgeon whose name is attached to a penetrating ulcer that connects the gastric antrum to the base of the duodenum—the double pyloric channel sign. Dragsted’s work was done before Marshall made the connection between H. pylori and peptic ulcer disease. Ulcers in the pyloric channel often manifest as gastric outlet obstruction after a chronic history of peptic ulcer disease. The manifestation of gastric outlet obstruction in a patient with no history of peptic ulcer disease is an ominous sign of possible malignancy.