[level-membership-for-gastroenterology-and-hepatology-category]CASE 190
History: A 32-year-old woman presents with mild jaundice.
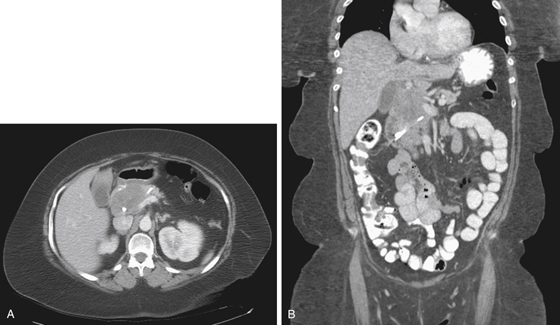
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
E. Peripancreatic lymphadenopathy
2. Which of the following statements regarding pancreatic lymphoma is true?
A. Pancreatic lymphoma represents less than 1% of pancreatic masses.
B. The uninvolved part of the pancreas becomes atrophic.
C. Pancreatic lymphoma is usually due to Hodgkin’s disease.
D. Diffuse lymphomatous infiltration results in high attenuation enlargement.
3. What finding is most suggestive of pancreatic lymphoma instead of carcinoma?
A. Absence of pancreatic duct dilation
4. What is the most common site of lymphomatous involvement of the gastrointestinal tract?
ANSWERS
CASE 190
Lymphoma of the Pancreatic Head
1. A, B, C, and E
2. A
3. A
4. B
References
Leite NP, Kased N, Hanna RF, et al: Cross-sectional imaging of extranodal involvement in abdominopelvic lymphoproliferative malignancies. Radiographics. 2007;27(6):1613-1635.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 169.
Comment
Primary pancreatic head lymphomas are rare; they account for about 0.5% of pancreatic masses. Secondary involvement of the pancreas by a non-Hodgkin’s lymphoma resulting from gross peripancreatic lymphadenopathy is more common. However, in cases such as the one shown here (see figures), in which the mass is entirely within the pancreatic substance and there is no evidence of lymphoma elsewhere, pancreatic lymphoma is a possible differential diagnosis. In this case, the lesion was a T-cell lymphoma. Most pancreatic lymphomas are B-cell lymphomas.
Diagnosis usually is confirmed by CT-guided needle aspiration or surgical pathology. Multidetector CT and routine and endoscopic ultrasound have also been useful in the diagnosis of pancreatic head masses. However, none of these imaging modalities can be considered specific. Nevertheless, multidetector CT imaging performed in this case shows a more homogeneous appearance, which might be expected with a hypovascular ductal adenocarcinoma. In addition, the small portion of the distal pancreas included in the images shows no evidence of pancreatic duct obstruction. The biliary duct obstruction that brought the patient to medical attention and resulted in stent placement completely resolved in a few days; this would be highly unlikely for the usual ductal carcinoma of the pancreas. All these observations, although not specific, might suggest alternative diagnostic possibilities. The incidence of lymphoma is increased in patients with AIDS, and the incidence of pancreatic lymphoma may also be increased.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 190
History: A 32-year-old woman presents with mild jaundice.
1. What should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
E. Peripancreatic lymphadenopathy
2. Which of the following statements regarding pancreatic lymphoma is true?
A. Pancreatic lymphoma represents less than 1% of pancreatic masses.
B. The uninvolved part of the pancreas becomes atrophic.
C. Pancreatic lymphoma is usually due to Hodgkin’s disease.
D. Diffuse lymphomatous infiltration results in high attenuation enlargement.
3. What finding is most suggestive of pancreatic lymphoma instead of carcinoma?
A. Absence of pancreatic duct dilation
[/not-level-membership-for-gastroenterology-and-hepatology-category]
