Procedure 19 Tendon Transfers for Ulnar Nerve Palsy
 See Video 15: Tendon Transfers for High Median and Ulnar Nerve Palsy
See Video 15: Tendon Transfers for High Median and Ulnar Nerve Palsy
Indications
 Delayed presentation (>1 year) of an ulnar nerve laceration
Delayed presentation (>1 year) of an ulnar nerve laceration
 Failed motor recovery after repair/reconstruction of the ulnar nerve
Failed motor recovery after repair/reconstruction of the ulnar nerve
 Failed motor recovery after release of ulnar nerve compression at Guyon canal or cubital tunnel
Failed motor recovery after release of ulnar nerve compression at Guyon canal or cubital tunnel
 Persistent motor weakness after completion of drug therapy in Hansen disease (leprosy)
Persistent motor weakness after completion of drug therapy in Hansen disease (leprosy)
 Neurologic disorders (for example, Charcot-Marie-Tooth disease, syringomyelia)
Neurologic disorders (for example, Charcot-Marie-Tooth disease, syringomyelia)
Examination/Imaging
Clinical Examination
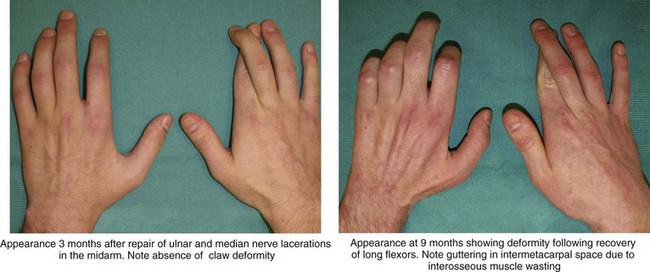
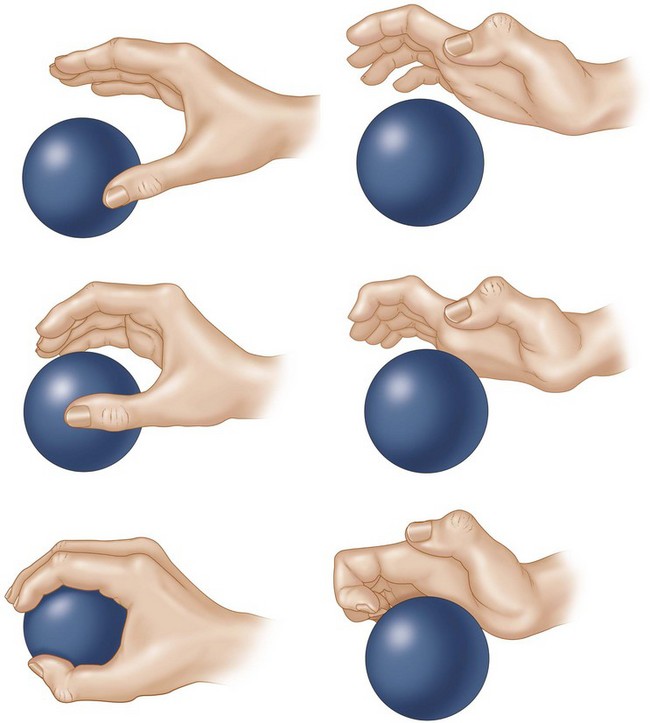
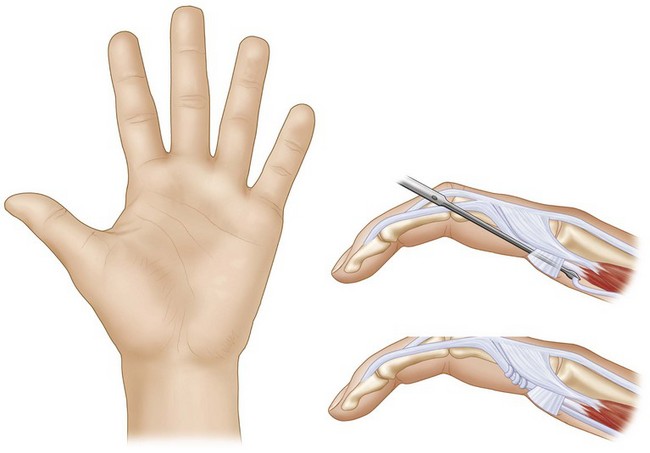
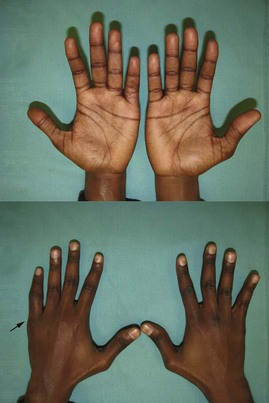
 Functional deficit: The loss of function in ulnar nerve palsy results from the claw deformity, which causes an abnormal pattern of finger flexion, weak thumb key pinch, small finger abduction deformity, and loss of ring and small finger distal interphalangeal (DIP) joint flexion (Fig. 19-1). However, these problems may not be functionally disabling in all patients, and some may require correction of only one aspect. It is important to determine this and then to set a sequence for the appropriate corrective procedures. It is better to correct the lack of DIP joint flexion first, followed by transfers for restoring thumb key pinch, and finally correction of the claw deformity because it is difficult to establish appropriate intrinsic plus posture of the hand.
Functional deficit: The loss of function in ulnar nerve palsy results from the claw deformity, which causes an abnormal pattern of finger flexion, weak thumb key pinch, small finger abduction deformity, and loss of ring and small finger distal interphalangeal (DIP) joint flexion (Fig. 19-1). However, these problems may not be functionally disabling in all patients, and some may require correction of only one aspect. It is important to determine this and then to set a sequence for the appropriate corrective procedures. It is better to correct the lack of DIP joint flexion first, followed by transfers for restoring thumb key pinch, and finally correction of the claw deformity because it is difficult to establish appropriate intrinsic plus posture of the hand.
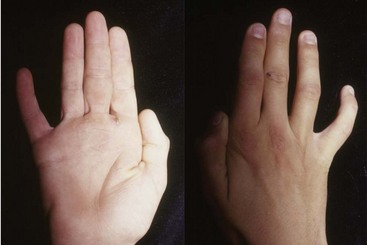
 Sensation: It is important to document the level of sensation in the thumb and the fingers preoperatively. Loss of sensation on the dorsoulnar aspect of the hand, which is innervated by the dorsal branch of ulnar nerve, can help differentiate a high ulnar nerve lesion (e.g., cubital tunnel compression) from a low ulnar nerve lesion (e.g., Guyon canal compression), which should have preserved sensation over the dorsal-ulnar hand (Fig. 19-7).
Sensation: It is important to document the level of sensation in the thumb and the fingers preoperatively. Loss of sensation on the dorsoulnar aspect of the hand, which is innervated by the dorsal branch of ulnar nerve, can help differentiate a high ulnar nerve lesion (e.g., cubital tunnel compression) from a low ulnar nerve lesion (e.g., Guyon canal compression), which should have preserved sensation over the dorsal-ulnar hand (Fig. 19-7).
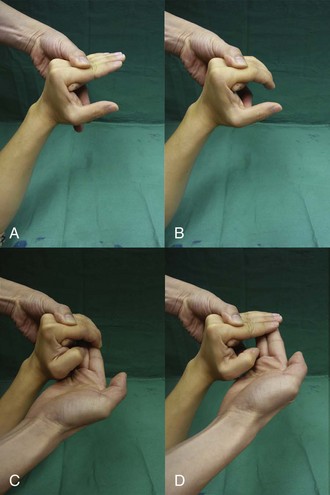
 Joints: To achieve a good result from the tendon transfer, patients must have good passive range of motion at the IP and the MCP joints. The most important aspect of assessment of an ulnar nerve palsy is determining whether the patient can extend the PIP joint with the examiner correcting the MCP joint hyperextension (Bouvier maneuver) (Fig. 19-8).
Joints: To achieve a good result from the tendon transfer, patients must have good passive range of motion at the IP and the MCP joints. The most important aspect of assessment of an ulnar nerve palsy is determining whether the patient can extend the PIP joint with the examiner correcting the MCP joint hyperextension (Bouvier maneuver) (Fig. 19-8).









Surgical Anatomy
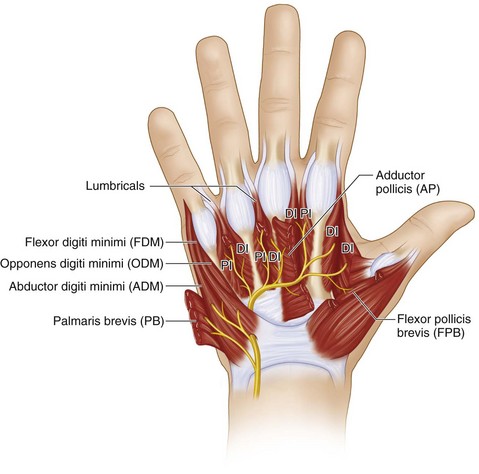
 The muscles affected after low ulnar nerve palsy are the four hypothenar muscles (abductor digitorum minimus [ADM], flexor digitorum minimus [FDM], opponens digitorum minimus [ODM], and palmaris brevis [PB]), seven interossei muscles (four dorsal and three palmar), third and fourth lumbricals, and two thenar muscles (adductor pollicis [AP] and the deep head of the flexor pollicis brevis [FPB]). All these muscles are innervated by the deep motor branch of the ulnar nerve (Fig. 19-10).
The muscles affected after low ulnar nerve palsy are the four hypothenar muscles (abductor digitorum minimus [ADM], flexor digitorum minimus [FDM], opponens digitorum minimus [ODM], and palmaris brevis [PB]), seven interossei muscles (four dorsal and three palmar), third and fourth lumbricals, and two thenar muscles (adductor pollicis [AP] and the deep head of the flexor pollicis brevis [FPB]). All these muscles are innervated by the deep motor branch of the ulnar nerve (Fig. 19-10).



Procedure 1—Static Correction of Claw Deformity with an MCP Joint Volar Plate Advancement
Exposures
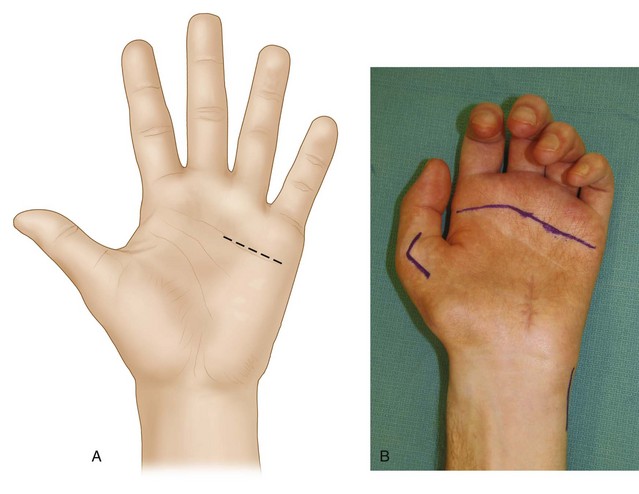
 A 3-cm transverse incision is made in line with the distal palmar crease overlying the ring and small finger MCP joints (Fig.19-11A and B).
A 3-cm transverse incision is made in line with the distal palmar crease overlying the ring and small finger MCP joints (Fig.19-11A and B).

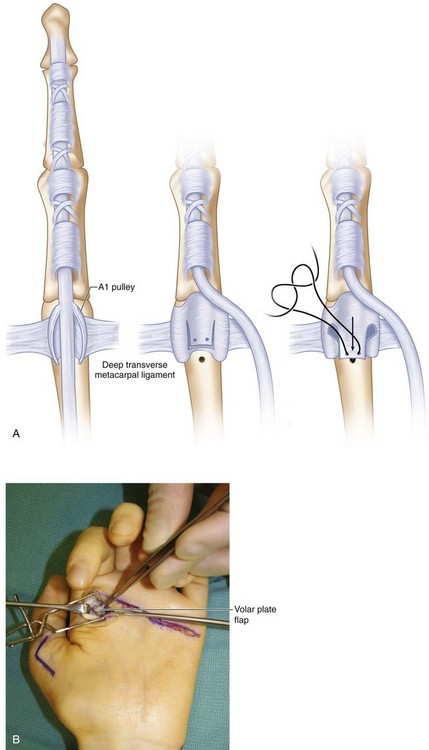
 The flexor tendon sheaths of the ring and small fingers are identified, and the A1 pulley is exposed (Fig. 19-12).
The flexor tendon sheaths of the ring and small fingers are identified, and the A1 pulley is exposed (Fig. 19-12).

Procedure
Step 1


Step 3

Step 4


Step 5

Step 5 Pearls
It is better to pass the sutures for all the fingers through the volar plate and tie them at the end instead of completing one finger and then proceeding to the next (Fig. 19-16). Passing the suture through the volar plate requires significant retraction, and an adjacent flexed finger will hinder this.
The suture must hold a good bite of the thick portion of the volar plate.

Step 6
 The wrist is maintained in a neutral position, and the ring finger capsular flap is sutured down to the neck of the metacarpal using the bone anchor sutures such that the MCP joint is flexed to about 45 to 50 degrees. The ring finger MCP joint should have slightly greater flexion compared with the long finger (Fig. 19-17).
The wrist is maintained in a neutral position, and the ring finger capsular flap is sutured down to the neck of the metacarpal using the bone anchor sutures such that the MCP joint is flexed to about 45 to 50 degrees. The ring finger MCP joint should have slightly greater flexion compared with the long finger (Fig. 19-17).


Step 6 Pearls
The amount of MCP joint flexion required to produce full PIP joint extension preoperatively can guide the surgeon regarding the degree of MCP joint flexion required intraoperatively.
Some authors recommend excising a 1.5-cm ellipse of skin (dermodesis) to prevent stretching the volar plate and overcorrecting the deformity.



Procedure 2—Dynamic Correction of Claw Deformity with Transfer of Ring Finger FDS
Exposures
 A Bruner-type incision centered over the PIP joint is made over the ring finger. Both neurovascular bundles are identified and retracted laterally to expose the flexor tendon sheath. Subsequently, the radial neurovascular bundle is retracted ulnarly, and a tissue plane is developed deep to it to expose the radial lateral band, which will receive the tendon transfer.
A Bruner-type incision centered over the PIP joint is made over the ring finger. Both neurovascular bundles are identified and retracted laterally to expose the flexor tendon sheath. Subsequently, the radial neurovascular bundle is retracted ulnarly, and a tissue plane is developed deep to it to expose the radial lateral band, which will receive the tendon transfer.

 A third 2-cm longitudinal incision is made on the radial aspect of the small finger proximal phalanx. The soft tissue is dissected to expose the radial lateral band (Fig. 19-18).
A third 2-cm longitudinal incision is made on the radial aspect of the small finger proximal phalanx. The soft tissue is dissected to expose the radial lateral band (Fig. 19-18).

Pearls
Additional lateral incisions can be made on the ulnar aspect of the index finger and radial aspect of the long finger if a claw correction of all four fingers is required.
The ulnar lateral band of the index and the radial lateral bands of the long, ring, and small fingers are chosen so that the tendon transfer can produce some adduction of these digits in addition to flexion at the MCP joint and extension at the PIP joint.
The long finger FDS should be used in patients with a high ulnar nerve palsy.
Step 1
 The A3 pulley of the ring finger is opened, and both slips of the FDS are identified.
The A3 pulley of the ring finger is opened, and both slips of the FDS are identified.


Step 1 Pearls
In patients who have a hyperextensible PIP joint, dividing the FDS proximal to the PIP joint can prevent the development of a swan neck deformity because the distal FDS insertion may be adherent to the volar plate and serve as a restraint. In patients who have a stiff PIP joint, the FDS should be divided distal to the PIP joint to prevent development of a flexion contracture.
Step 2
 The ring finger FDS tendon is identified at the midpalmar incision and withdrawn out of the incision.
The ring finger FDS tendon is identified at the midpalmar incision and withdrawn out of the incision.
 The distal split in the FDS tendon is completed all the way in the visible portion of the tendon (Fig. 19-19).
The distal split in the FDS tendon is completed all the way in the visible portion of the tendon (Fig. 19-19).
Step 3
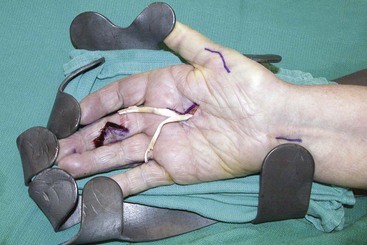
 The origin of the lumbrical muscle from the FDP is identified. A mosquito forceps or a tendon passer is passed from the palmar incision along the lumbrical through the lumbrical canal (remaining superficial/palmar to the deep transverse metacarpal ligament) to exit on the incision made on the radial side of the small finger (Fig. 19-21).
The origin of the lumbrical muscle from the FDP is identified. A mosquito forceps or a tendon passer is passed from the palmar incision along the lumbrical through the lumbrical canal (remaining superficial/palmar to the deep transverse metacarpal ligament) to exit on the incision made on the radial side of the small finger (Fig. 19-21).

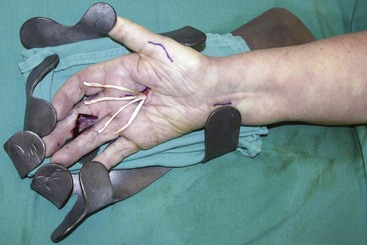
 The same procedure is repeated to bring the radial slip of the FDS through the lumbrical canal on the radial aspect of the ring finger (Fig. 19-22).
The same procedure is repeated to bring the radial slip of the FDS through the lumbrical canal on the radial aspect of the ring finger (Fig. 19-22).


Step 5
 The forearm is pronated, and a rolled-up towel is placed in the palm so that the wrist is in neutral position and the MCP joints are flexed beyond the rolled towel.
The forearm is pronated, and a rolled-up towel is placed in the palm so that the wrist is in neutral position and the MCP joints are flexed beyond the rolled towel.


Step 5 Pearls
The MCP joint cascade can be corrected by tightening or loosening the FDS attachment to the lateral band.
The desired tension is to keep the MCP joint in about 60 to 70 degrees of flexion and the IP joint in full extension, with the wrist at about 20 degrees of extension. In most cases, the ideal tension cannot be established because of the large amount of excursion of the FDS, which reaches 70 mm. Therefore, getting close to this posture is acceptable because the FDS, which is considered a smart tendon because of its excursion, can modulate the tension to reach an acceptable posture (Fig. 19-23).




Procedure 3—Restoration of Thumb Adduction with an ECRB Tendon Transfer
Exposures
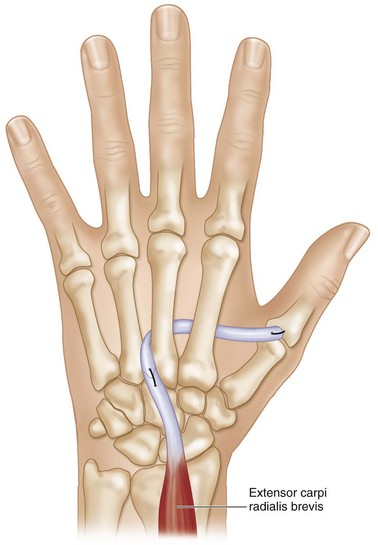
 A 3-cm longitudinal incision is made starting at the base of the ulnar aspect of the long finger metacarpal and extending distally. The soft tissue is dissected, and the ECRB is exposed at its insertion onto the base of the long metacarpal. Distally, the dorsal interosseous fascia overlying the interspace between the long and ring metacarpals is divided, and interosseous muscles are exposed (Fig. 19-24).
A 3-cm longitudinal incision is made starting at the base of the ulnar aspect of the long finger metacarpal and extending distally. The soft tissue is dissected, and the ECRB is exposed at its insertion onto the base of the long metacarpal. Distally, the dorsal interosseous fascia overlying the interspace between the long and ring metacarpals is divided, and interosseous muscles are exposed (Fig. 19-24).






Step 3



Step 4



Step 6
 A curved hemostat is used to make a subcutaneous tunnel from the ulnar aspect of the thumb MCP joint to the third to fourth intermetacarpal space. This tunnel is made superficial (palmar) to the adductor pollicis but deep (dorsal) to the flexor tendons (Fig. 19-27).
A curved hemostat is used to make a subcutaneous tunnel from the ulnar aspect of the thumb MCP joint to the third to fourth intermetacarpal space. This tunnel is made superficial (palmar) to the adductor pollicis but deep (dorsal) to the flexor tendons (Fig. 19-27).
 The hemostat then grabs the ECRB extended by the PL graft and brings it out to the thumb.
The hemostat then grabs the ECRB extended by the PL graft and brings it out to the thumb.





Procedure 4—Correction of Abduction Deformity (Wartenberg Sign) of Small Finger
Exposures
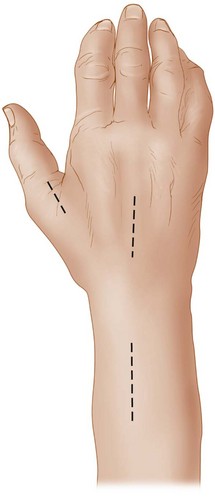
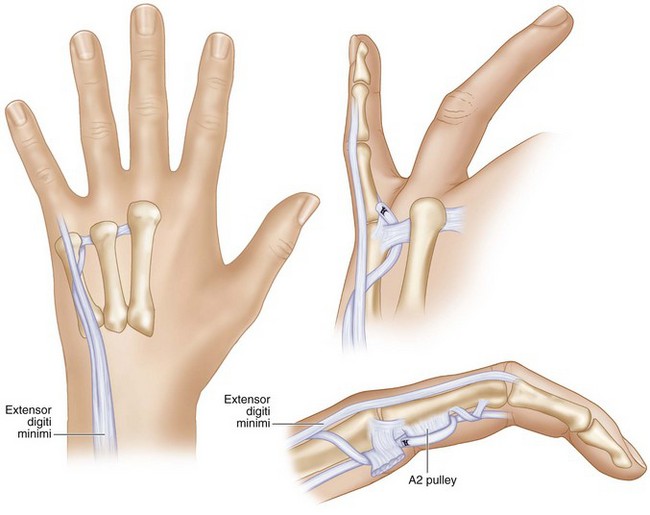
 A 3-cm chevron-shaped incision with the apex directed ulnarly is made over the dorsal aspect of the small finger MCP joint. The skin and soft tissue are dissected to expose the tendon of the EDM (Figs. 19-29 and 19-30).
A 3-cm chevron-shaped incision with the apex directed ulnarly is made over the dorsal aspect of the small finger MCP joint. The skin and soft tissue are dissected to expose the tendon of the EDM (Figs. 19-29 and 19-30).



Step 1


Step 2
 The tendon is sutured to the phalangeal attachment of the radial collateral ligament with the wrist in neutral position with the assistant holding the small finger adducted (Fig. 19-31).
The tendon is sutured to the phalangeal attachment of the radial collateral ligament with the wrist in neutral position with the assistant holding the small finger adducted (Fig. 19-31).
Step 2 Pearls
The transfer of the ulnar half of the EDM tendon to the radial collateral ligament is useful in patients with low ulnar nerve palsy who have an abduction deformity but do not have clawing or have clawing that has been corrected by a previous transfer.
In patients who have clawing, an additional 2.5-cm oblique palmar incision is made between the distal palmar crease and the proximal digital crease of the small finger. The common digital neurovascular bundle is identified and retracted radially to expose the deep transverse metacarpal ligament. The EDM tendon is retrieved using a hemostat and passed from dorsum to palmar between the fourth and fifth metacarpals, remaining palmar to the deep transverse metacarpal ligament. It is passed through a slit made in the proximal half of the A2 pulley and sutured to itself with the assistant holding the wrist in neutral position, the MCP joint in 20 degrees of flexion, and the small finger adducted (see Fig. 19-31).

Postoperative Care and Expected Outcomes
 A splint is applied that keeps the small and ring fingers MCP joints in 60 to 70 degrees of flexion and the wrist in neutral position. The IP joints are left free.
A splint is applied that keeps the small and ring fingers MCP joints in 60 to 70 degrees of flexion and the wrist in neutral position. The IP joints are left free.
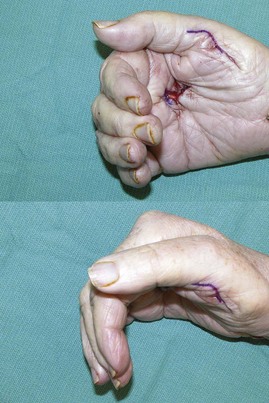
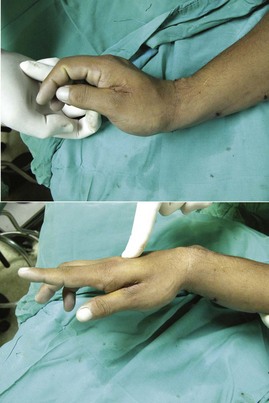
 Ten days after surgery, the wound is inspected, sutures are removed, and the position is maintained using a removable splint that the patient will wear for another 4 weeks, provided that the patient is reliable in keeping the splint on at all times, except in the daily cleaning of the hand. Thereafter, the patient is encouraged to move the MCP joint, and a protective removable splint is also provided for night wear and general protection for the next 4 weeks. The protective splint is discontinued 2 months after surgery, and the patient is allowed unrestricted activity (Fig. 19-32).
Ten days after surgery, the wound is inspected, sutures are removed, and the position is maintained using a removable splint that the patient will wear for another 4 weeks, provided that the patient is reliable in keeping the splint on at all times, except in the daily cleaning of the hand. Thereafter, the patient is encouraged to move the MCP joint, and a protective removable splint is also provided for night wear and general protection for the next 4 weeks. The protective splint is discontinued 2 months after surgery, and the patient is allowed unrestricted activity (Fig. 19-32).
 This is a simple procedure to correct an annoying disability.
This is a simple procedure to correct an annoying disability.
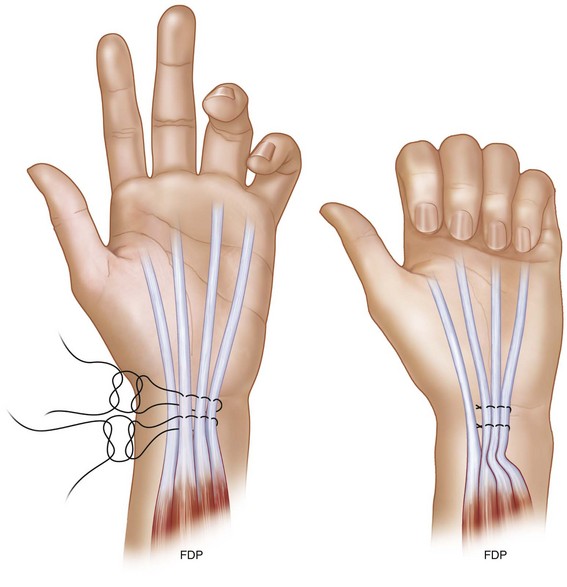
Procedure 5—Side-to-Side FDP Transfer for Restoration of Ring and Small Finger DIP Joint Flexion Strength (High Ulnar Palsy)
Exposures
 A 4-cm longitudinal incision is made 2 cm proximal to the wrist crease ulnar and parallel to the tendon of the palmaris longus. The antebrachial fascia is divided, and the PL tendon is retracted radially. The median nerve is identified and retracted radially. Next, the FDS tendons to the ring and long finger are identified and retracted radially. Immediately below are the FDS tendons to the small and index fingers. The index FDS is retracted radially, and the small FDS is retracted ulnarly. This exposes the four FDP tendons.
A 4-cm longitudinal incision is made 2 cm proximal to the wrist crease ulnar and parallel to the tendon of the palmaris longus. The antebrachial fascia is divided, and the PL tendon is retracted radially. The median nerve is identified and retracted radially. Next, the FDS tendons to the ring and long finger are identified and retracted radially. Immediately below are the FDS tendons to the small and index fingers. The index FDS is retracted radially, and the small FDS is retracted ulnarly. This exposes the four FDP tendons.






Hastings H, McCollam SM. Flexor digitorum superficialis lasso tendon transfer in isolated ulnar nerve palsy: a functional evaluation. J Hand Surg [Am]. 1994;19:275-280.
Ozkan T, Ozer K, Gulgonen A. Three tendon transfer methods in reconstruction of ulnar nerve palsy. J Hand Surg [Am]. 2003;28:35-43.
Smith RJ. Extensor carpi radialis brevis tendon transfer for thumb adduction: a study of power pinch. J Hand Surg [Am]. 1983;8:4-15.
Trevett MC, Tuson C, de Jager LT, Juon JM. The functional results of ulnar nerve repair: defining the indications for tendon transfer. J Hand Surg [Br]. 1995;20:444-446.


