Autotransfusion
PREREQUISITE NURSING KNOWLEDGE
• Understanding of transfusion and intravenous therapy and fluid balance is necessary.
• Significant blood loss, related systemic hypoperfusion, and the associated decrease in oxygen-carrying capacity, with its impact on hypoxemia, often necessitate the replacement of blood with whole blood or packed cells. In appropriate patient populations (trauma, cardiovascular, or orthopedic surgical patients), autotransfusion should be considered as the need to replace blood becomes apparent.
• Autotransfusion is commonly used for trauma victims and for patients undergoing cardiovascular and orthopedic procedures; it reduces the need for banked blood transfusions with the inherent risks of transfusion reactions and disease transmission.
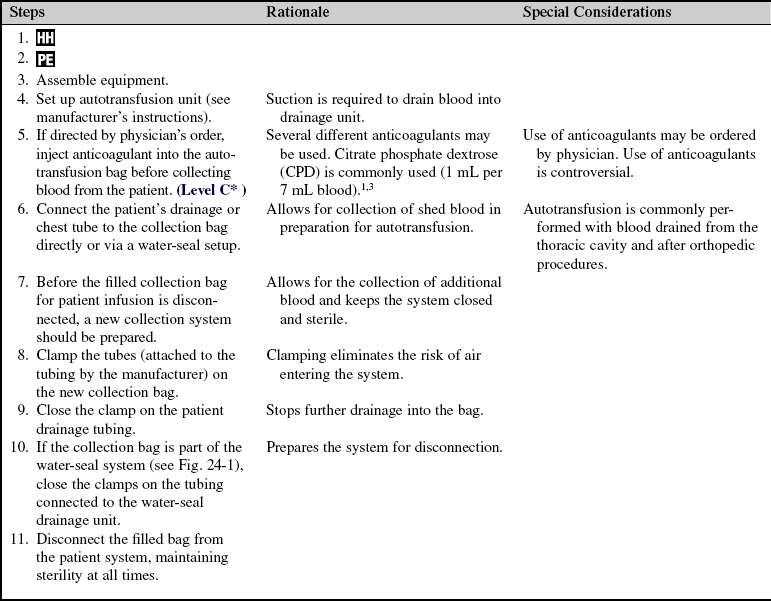
• A variety of autotransfusion devices are available. An autotransfusion system may be a standard water-seal chest drainage system (see Fig. 24-1, A), a separate autotransfusion setup, or a modified chest drainage autotransfusion system. In addition, continuous and intermittent systems are available. A continuous system has an intravenous line connected directly from the drainage unit collection chamber to the patient. An intermittent system uses a blood collection bag in-line between the chest tube and the collection chamber.
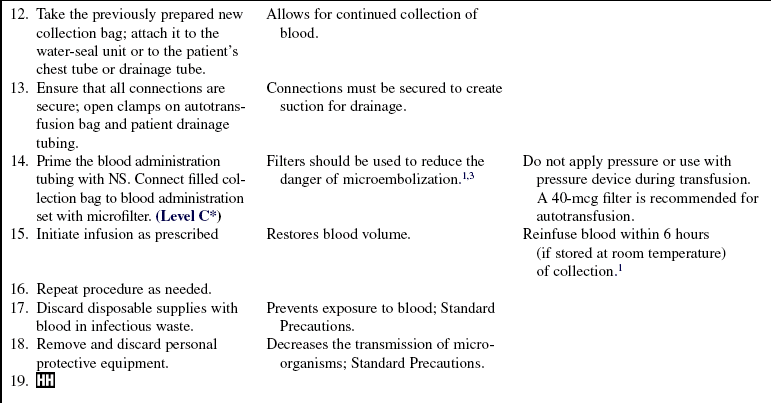
• Many disposable systems available today have the ability to act as a reservoir for autotransfusion if the need arises. To initiate autotransfusion, the autotransfusion bag is disconnected from the disposable system and connected to the saline solution–filled blood administration tubing. Nurses should gain familiarity with their institution’s autotransfusion system and policies.
• Indications for autotransfusion in the appropriate patient populations include active bleeding (greater than 100 mL/hr) and the accumulation of greater than 300 mL of drainage in the collection chamber.
• Contraindications to autotransfusion include the following:





• Any contraindications to autotransfusion are overruled in the presence of exsanguinating hemorrhage in the absence of an adequate supply of banked blood.
• As with banked blood, patients may refuse to receive autologous blood based on religious beliefs.
• Informed consent should be obtained in nonemergency situations.
 Rationale: Information enhances patient and family understanding and decreases anxiety.
Rationale: Information enhances patient and family understanding and decreases anxiety.PATIENT ASSESSMENT AND PREPARATION
Patient Assessment








Patient Preparation
• Verify correct patient using two identifiers.  Rationale: Prior to performing a procedure the nurse should ensure the correct identification of the patient for the intended intervention.
Rationale: Prior to performing a procedure the nurse should ensure the correct identification of the patient for the intended intervention.
• Ensure that the patient understands preprocedural teachings. Answer questions as they arise, and reinforce information as needed.  Rationale: This communication evaluates and reinforces understanding of previously taught information.
Rationale: This communication evaluates and reinforces understanding of previously taught information.
References
![]() 1. American Association of Blood Banks, Guidelines for blood recovery and reinfusion in surgery and trauma . American Association of Blood Banks, Bethesda, MD, 1997.
1. American Association of Blood Banks, Guidelines for blood recovery and reinfusion in surgery and trauma . American Association of Blood Banks, Bethesda, MD, 1997.
2. American Association of Blood Banks. Technical manual, ed 16. Bethesda, MD: American Association of Blood Banks; 2008.
![]() 3. Purcell, TB. Autotransfusion. In: Roberts JR, Hedges JR, eds. Clinical procedures in emergency medicine. ed 4. Philadelphia: Saunders; 2004:410–426.
3. Purcell, TB. Autotransfusion. In: Roberts JR, Hedges JR, eds. Clinical procedures in emergency medicine. ed 4. Philadelphia: Saunders; 2004:410–426.
American Association of Blood Banks Guidance for standards for perioperative autologous blood collection and administration. American Association of Blood Banks, Bethesda, MD, 2002.
Brown, M, Whalen, PK, Red blood cell transfusion in critically ill patients. emerging risks and alternatives. Crit Care Nurse 2000; 1–14. [(Suppl)].
Cross, MH, Autotransfusion in cardiac surgery . Perfusion 2001; 16:391–400.
Dial, S, Nguyen, D, Menzies, D, Autotransfusion of shed mediastinal blood. a risk factor for mediastinitis after cardiac surgery? Results of a cluster investigation. Chest. 2003; 124(5):1847–1851.
Ley, SJ, Intraoperative and postoperative blood salvage . AACN Clin Issues 1996; 7:238–248.
Oeltjen, AM, Santrach PJ, Autologous transfusion techniques. J Intraven Nurs . 1997; 20:305–310.
Sirvinskas, E, Veikutiene, A, Benetis, R, et al. Influence of early re-infusion of autologous shed mediastinal blood on clinical outcome after cardiac surgery. Perfusion. 2007; 22(5):345–352.
Weniger, J, von der Emde J, Schricker, K, et al. Autotransfusion of drainage blood after heart surgery. Langenbecks Archiv Für Chirurgie. 1980; 351(4):229–241. [(author’s transl)].
