Published on 02/03/2015 by admin
Filed under Internal Medicine
Last modified 22/04/2025
This article have been viewed 1484 times
Case 19
A 65-year-old man had abnormalities on his electrocardiogram (ECG) at a routine outpatient office visit with his primary physician. He was referred for exercise stress/rest myocardial perfusion imaging.
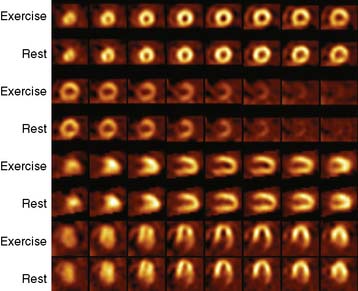
He exercised for 9 minutes, 15 seconds, achieving 10 METs with Bruce protocol. His heart rate changed from 55 beats/min to 135 beats/min (achieving 87% target) and blood pressure from 150/70 to 190/90 mm Hg. Resting ECG showed sinus rhythm with left anterior fascicular block and nonspecific ST-T changes in limb leads. No chest pain or ST-segment change occurred on stress. Patient underwent stress-rest 99mTc-sestamibi perfusion imaging.
(Video 1a)
(Video 1b)
(Fig. 1)
(Fig. 2a)
(Fig. 2b)
(Fig. 2c)
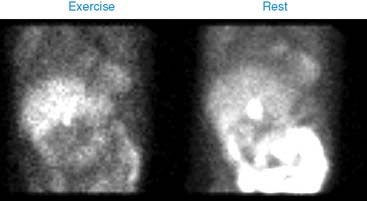
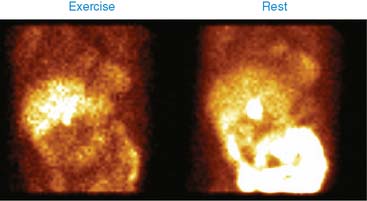
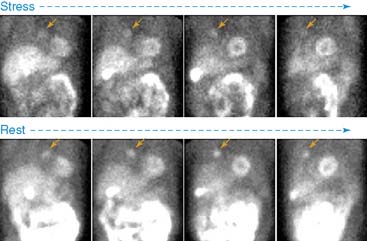
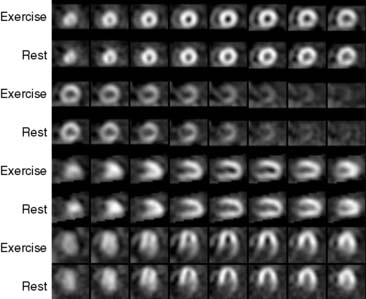
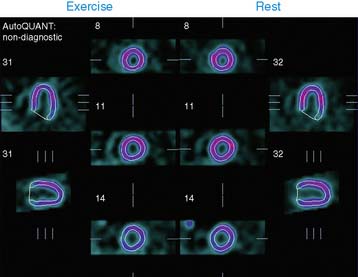
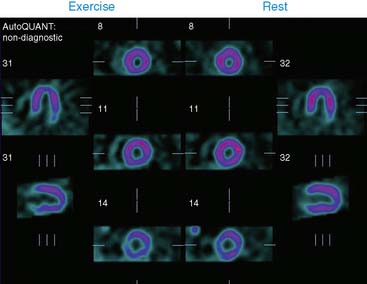
Perfusion imaging showed a small area of perfusion abnormality involving the inferolateral wall, which was reversible on rest images. Left ventricular ejection fraction (LVEF) was 61%. There was a large nodular area of radiotracer uptake in the right lung in the mediastinum, which was suspicious for thymoma, ectopic thyroid tissue, or some other malignant mass such as lymphoma.
(Video 2a)
Coronary angiogram showed bilateral coronary calcifications, with luminal irregularities in distal left anterior descending (LAD) and proximal large first obtuse marginal, and focal 50% stenosis in proximal right coronary artery (RCA).
Computed tomography scan of the patient’s chest showed an anterior mediastinal mass measuring 3.8 × 2.5 cm. He underwent thoracotomy and excision of the mediastinal mass, which proved to be a thymoma.
(Video 2b)
Clinical Nuclear Cardiology State of the Art and Future Directio
WhatsApp us